

Effect of initiation of antiretroviral drugs for HIV prevention or treatment on the vaginal microbiome of pregnant women in Malawi
- PMID: 40287413
- PMCID: PMC12033299
- DOI: 10.1038/s41522-025-00697-8
Effect of initiation of antiretroviral drugs for HIV prevention or treatment on the vaginal microbiome of pregnant women in Malawi
Abstract
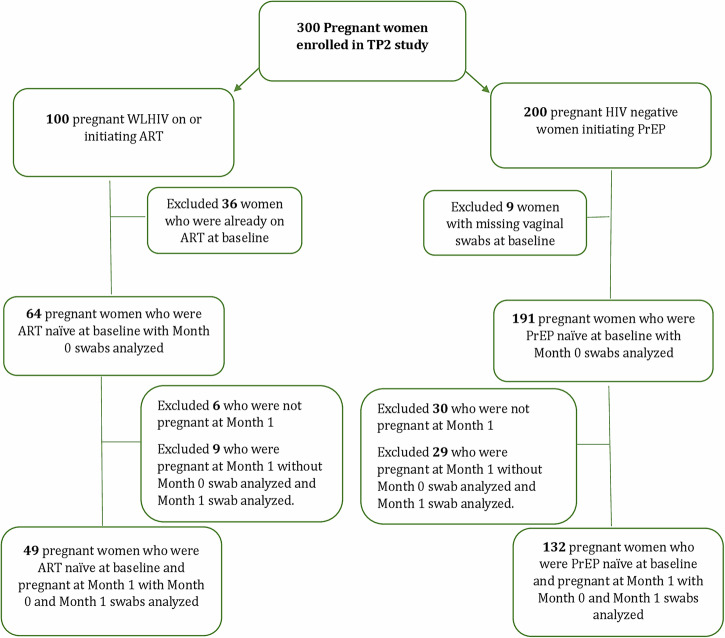
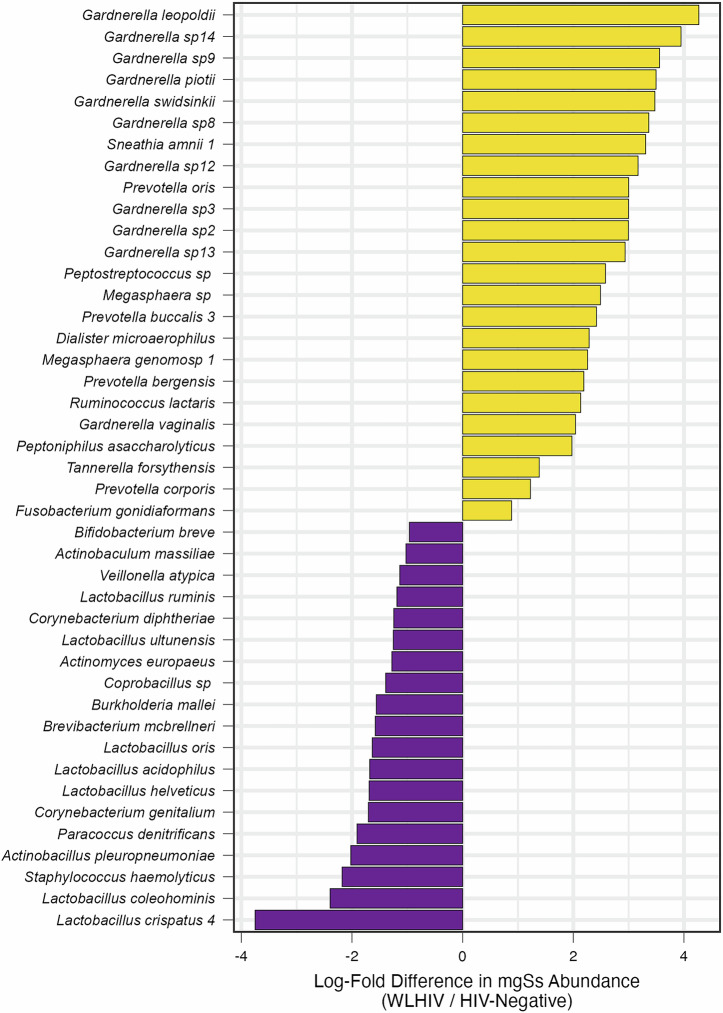
Lack of Lactobacillus and/or dysbiosis is linked to spontaneous preterm birth (sPTB). The impact of antiretrovirals (ARVs) for HIV treatment or prevention on the vaginal microbiome during pregnancy remains unclear. We examined vaginal microbiome changes in pregnant women in Lilongwe, Malawi. Women living with HIV (WLHIV) initiated antiretroviral therapy (ART), while HIV-negative women began oral pre-exposure prophylaxis (PrEP). Of 255 participants (191 HIV-negative, 64 WLHIV) who provided baseline vaginal swabs, 181 provided follow-up swabs one month after ARV initiation. At enrollment, WLHIV had higher Shannon diversity and were more likely to have CST IV-B than CST I or III. After ARV initiation, α-diversity decreased in WLHIV but increased in HIV-negative women. Women initiating PrEP had a lower risk of sPTB compared to WLHIV initiating ART, but transitioning to CST IV during pregnancy increased the odds of sPTB. Larger studies are needed to explore ARV impact on pregnancy outcomes.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: J.R. is co-founder of LUCA Biologics, a biotechnology company focusing on translating microbiome research into live biotherapeutics drugs for women’s health. The other authors declare no competing interests.
Figures






References
-
- Kimberlin, D. F. & Andrews, W. W. Bacterial vaginosis: association with adverse pregnancy outcome. Semin Perinatol.22, 242–250 (1998). - PubMed
-
- Atowoju, I., Dawer, P., Asrani, M. & Panjiyar, B. Impact of maternal HIV infection on perinatal outcomes: A systematic review. Int J. Gynaecol. Obstet.166, 35–43 (2024). - PubMed
-
- Tshivuila-Matala, C. O. O. et al. Adverse perinatal outcomes associated with antiretroviral therapy regimens: systematic review and network meta-analysis. AIDS34, 1643–1656 (2020). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
