

Characteristics of chronic subdural haematomas related to DOACs vs warfarin
- PMID: 40287645
- PMCID: PMC12034213
- DOI: 10.1186/s12883-025-04134-3
Characteristics of chronic subdural haematomas related to DOACs vs warfarin
Abstract
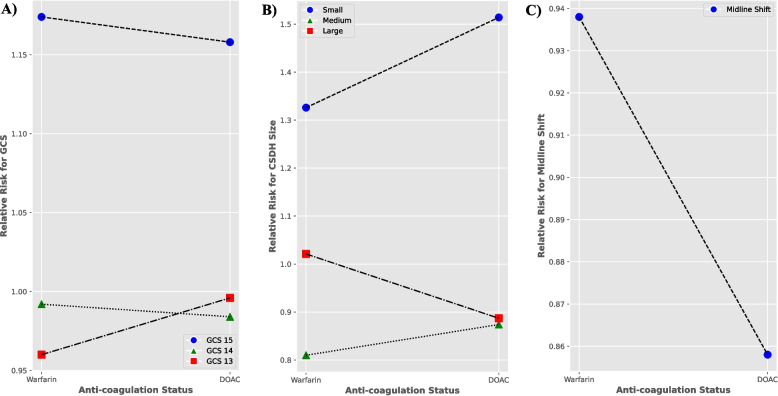
Objectives: The aim of this study was to investigate the effects of anticoagulation with DOACs and warfarin on the characteristics of chronic subdural hematomas (CSDHs), specifically, the size of the hematomas, the presence of midline shift and the effect on consciousness levels, measured via the Glasgow Coma Scale (GCS).
Methods: A multi-centre retrospective case series analysis from January 2015 to May 2020 was conducted. Patients who were anticoagulated with DOACs and warfarin were of primary interest. The CSDH characteristics that were focussed on included the size of the CSDH, midline shift and GCS. Chi-squared analysis and independent t-tests were conducted for inter-variable analysis. Relative risk was also calculated.
Results: Two thousand, six hundred seventy-five patients across two tertiary neurosurgical units referred with CSDHs were included in the analysis. 1799 patients were male (67.3%), with a mean age of 78.5 years. 905 patients (33.8%) were on antithrombotic therapy, with 298 patients (11.1%) on warfarin and 203 patients (7.6%) on DOACs. There were statistically significant associations between the type of antithrombotic medication and both midline shift and size of the CSDH (p < 0.0001), but not GCS (p = 0.1956). No significant difference in relative risk (RR) for impaired GCS was found between DOACs and warfarin (1.158 vs 1.174 respectively). Relative risk analysis revealed a safer profile for DOACs, with a lower risk of developing a larger sized hematoma (RR 0.887 v 1.021) and a reduced likelihood of midline shift (RR 0.858 VS 0.938), which was supported by effect size analysis using odd's ratios. Comparative risk analysis between DOACs and warfarin further demonstrated a higher risk of midline shift for patients on warfarin (RR 1.431), that trended towards statistical significance (p = 0.0511, 95% confidence interval 0.998-2.05).
Conclusions: For CSDH patients, DOACs may potentially be a safer method of anticoagulation as opposed to warfarin as they appear to be linked to the development of smaller sized hematomas and reduced midline shift, although there was no significant difference in GCS between the groups. These features are known to reduce the risk of needing neurosurgical intervention for CSDH. This is important in influencing the management of an increasingly ageing, multi-morbid population on increasing amounts of anticoagulation medication.
Keywords: Anti-coagulation; Chronic Subdural Hematoma; DOAC; Warfarin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Consent to participate was waived by the Northwest Research and Innovation Institutional Review board, reference number: 22HIP11. All subsequent methods were performed in accordance with the relevant local guidelines and regulations. The study further adhered to the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
