

Fully endoscopic keyhole approach for intracranial aneurysm clipping: clinical outcomes and technical note
- PMID: 40287737
- PMCID: PMC12032781
- DOI: 10.1186/s40001-025-02594-4
Fully endoscopic keyhole approach for intracranial aneurysm clipping: clinical outcomes and technical note
Abstract
Background: Surgical clipping is often utilized to treat intracranial aneurysms. The application of the endoscopy and keyhole approach in neurosurgery is increasing gradually in intracranial aneurysm occlusion. The aim of this study is to evaluate the role of fully endoscopic keyhole approach in clipping of intracranial aneurysms.
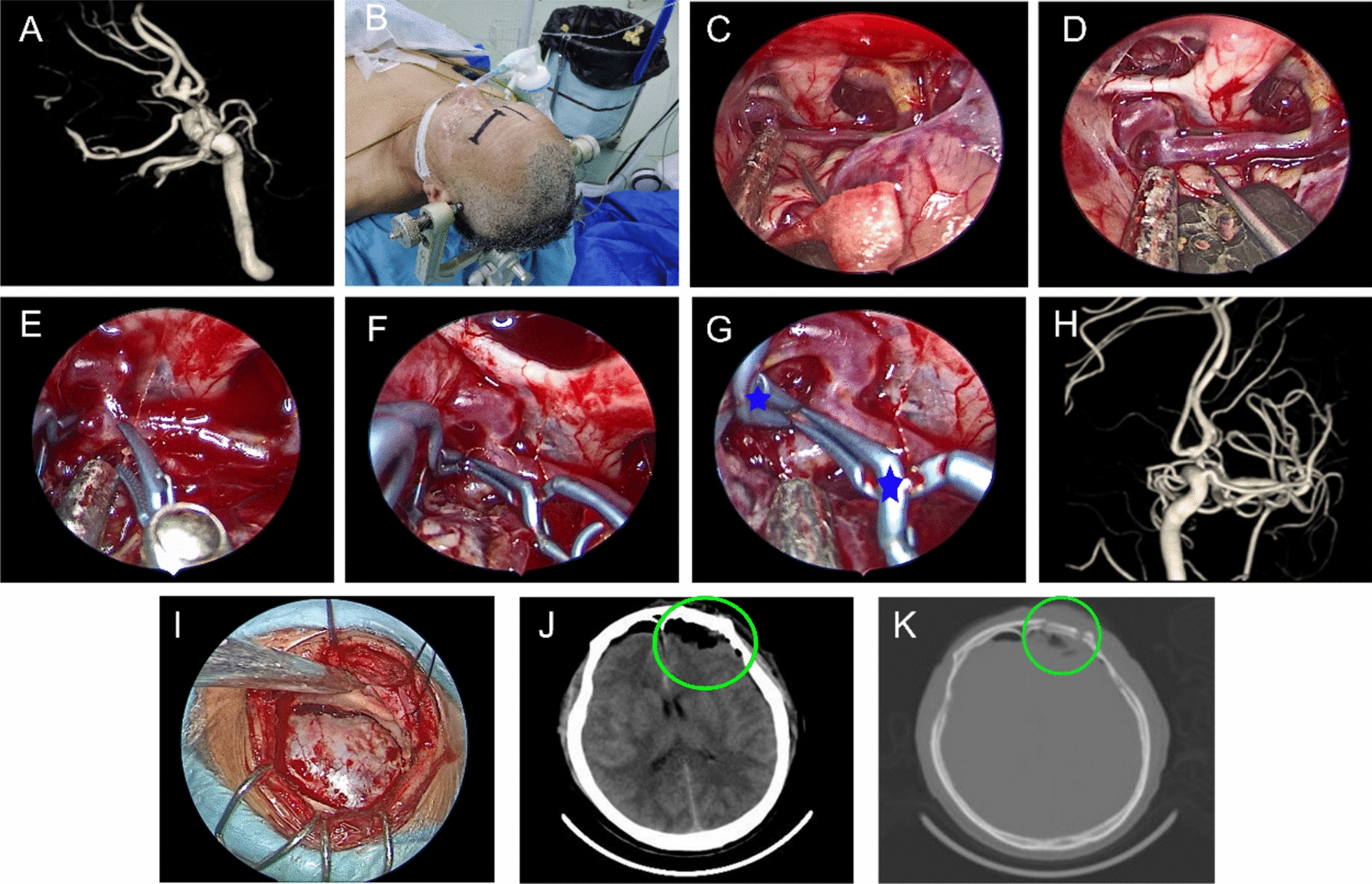
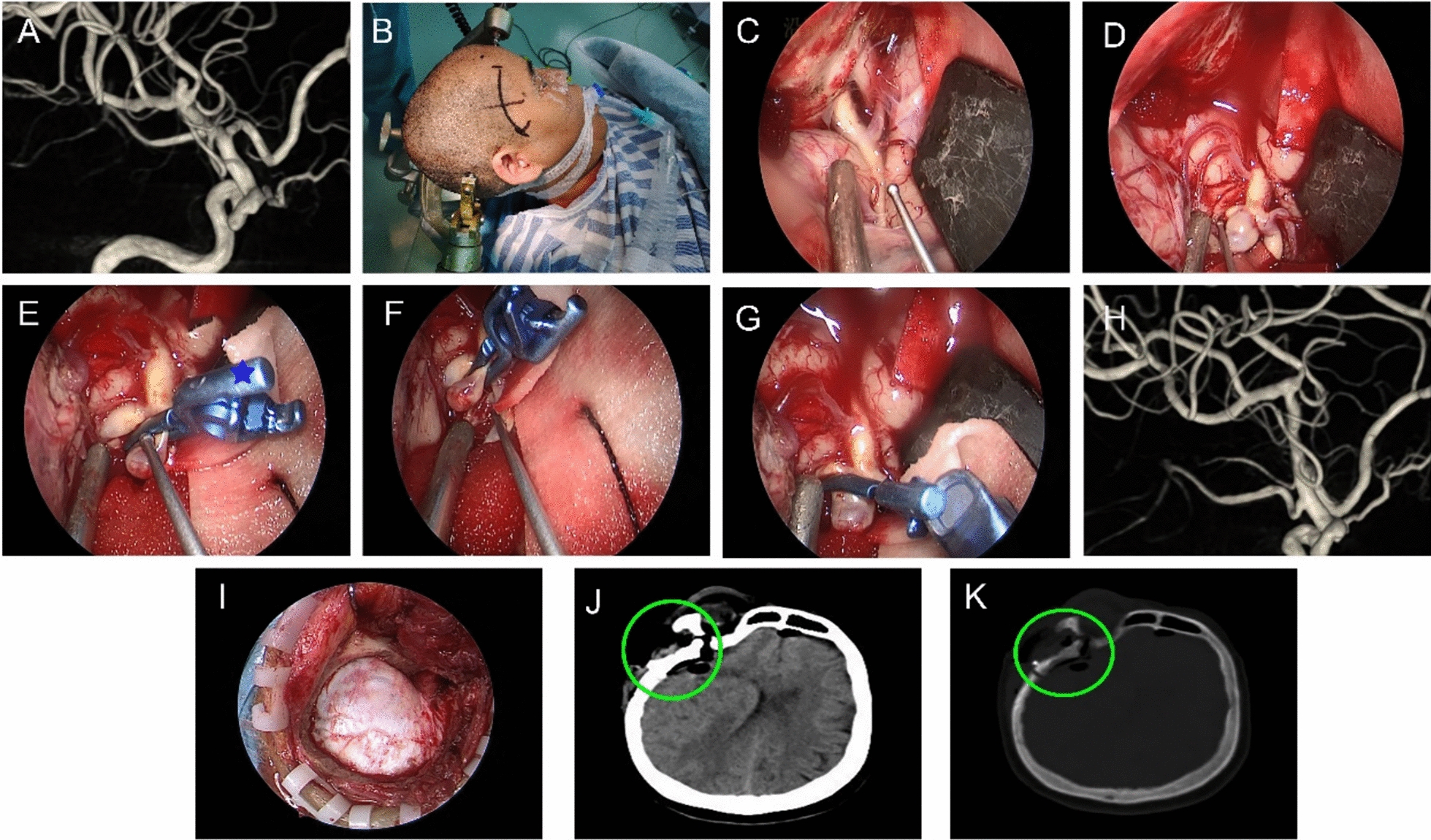
Methods: We retrospectively analyzed four cases of intracranial aneurysms, including three cases of middle cerebral artery bifurcation aneurysms (M1) and one case of anterior communicating aneurysms (ACoA). Among them, the anterior communicating aneurysm underwent fully endoscopic clipping via supraorbital keyhole approach and the middle cerebral aneurysms underwent fully endoscopic clipping via mini-pterional keyhole approach. The clipped aneurysms were evaluated by Digital Subtraction Angiography (DSA).
Results: All patients had satisfactory cerebral aneurysm clipping via the endoscopic keyhole approach. There was no cerebral hemorrhage, cerebral infarction, cerebral vasospasm. One case of intracranial infection was cured by active anti-infection. No recurrence of aneurysms after 6 months of follow-up.
Conclusion: With the advantages of the endoscopy and keyhole approach, the excellent visual field of the endoscope can reduce the influence of intracranial aneurysmal neck residual and perforating vessel. However, endoscopic clipping of intracranial aneurysms in narrow corridors requires a learning curve.
Keywords: Clipping; Endoscopy; Intracranial aneurysms; Keyhole approach; Minimally invasive.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Research Ethics Committee of Bengbu Medical University. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
