

Beyond the "string of beads": case-based exploration of diagnostic pitfalls and solutions in reversible cerebral vasoconstriction syndrome
- PMID: 40289076
- PMCID: PMC12036309
- DOI: 10.1186/s10194-025-01978-5
Beyond the "string of beads": case-based exploration of diagnostic pitfalls and solutions in reversible cerebral vasoconstriction syndrome
Abstract
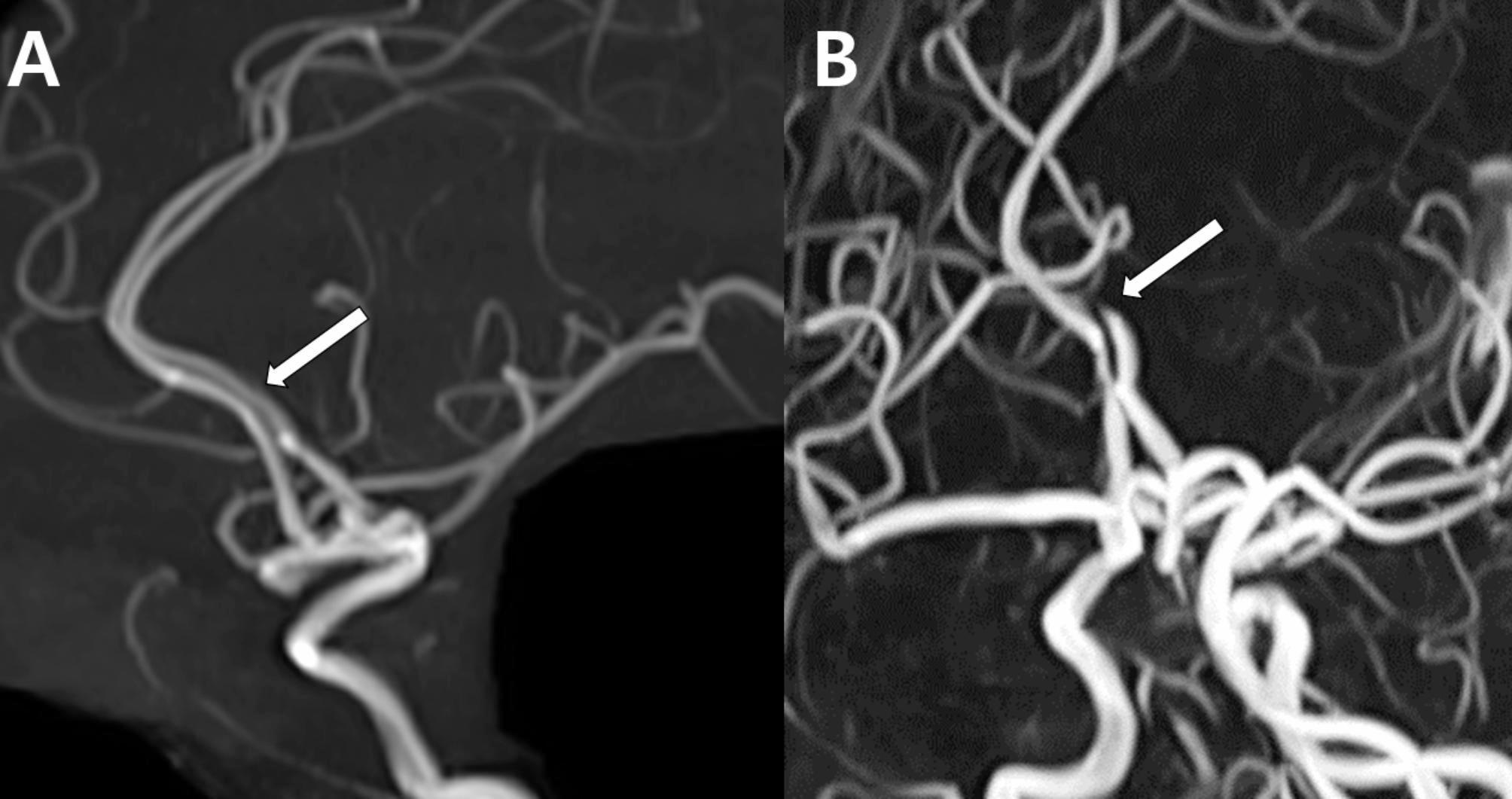
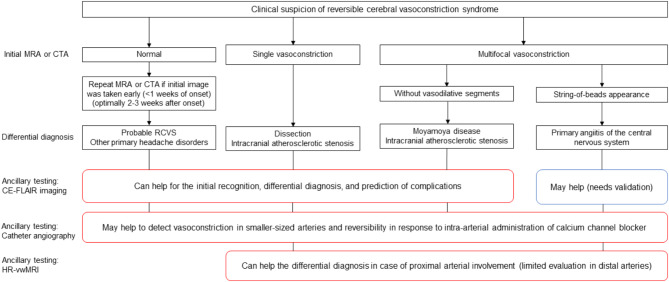
Background: The diagnosis of reversible cerebral vasoconstriction syndrome (RCVS) is challenging due to its varied clinical manifestations and imaging findings. While it typically presents with a sudden, severe thunderclap headache and multifocal constriction of the cerebral arteries, the wide spectrum of radiological presentations may complicate the diagnosis.
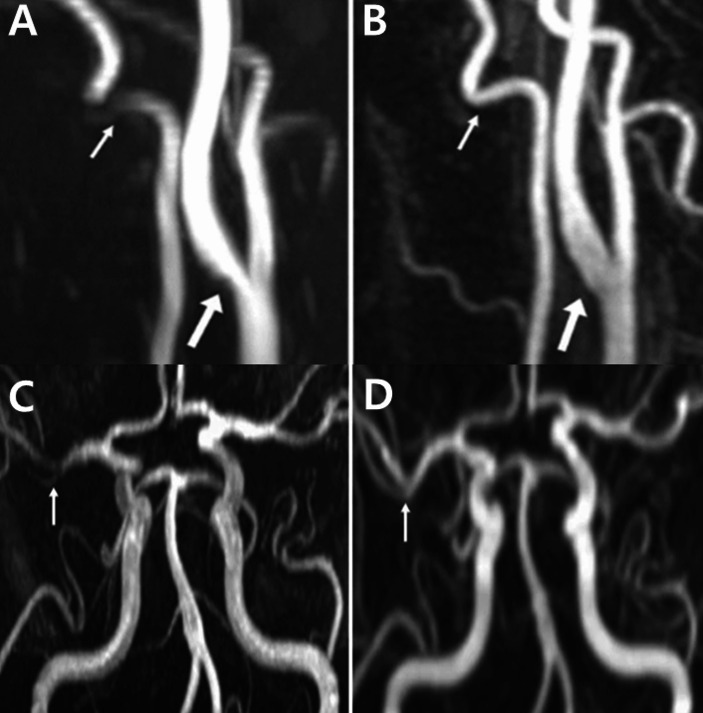
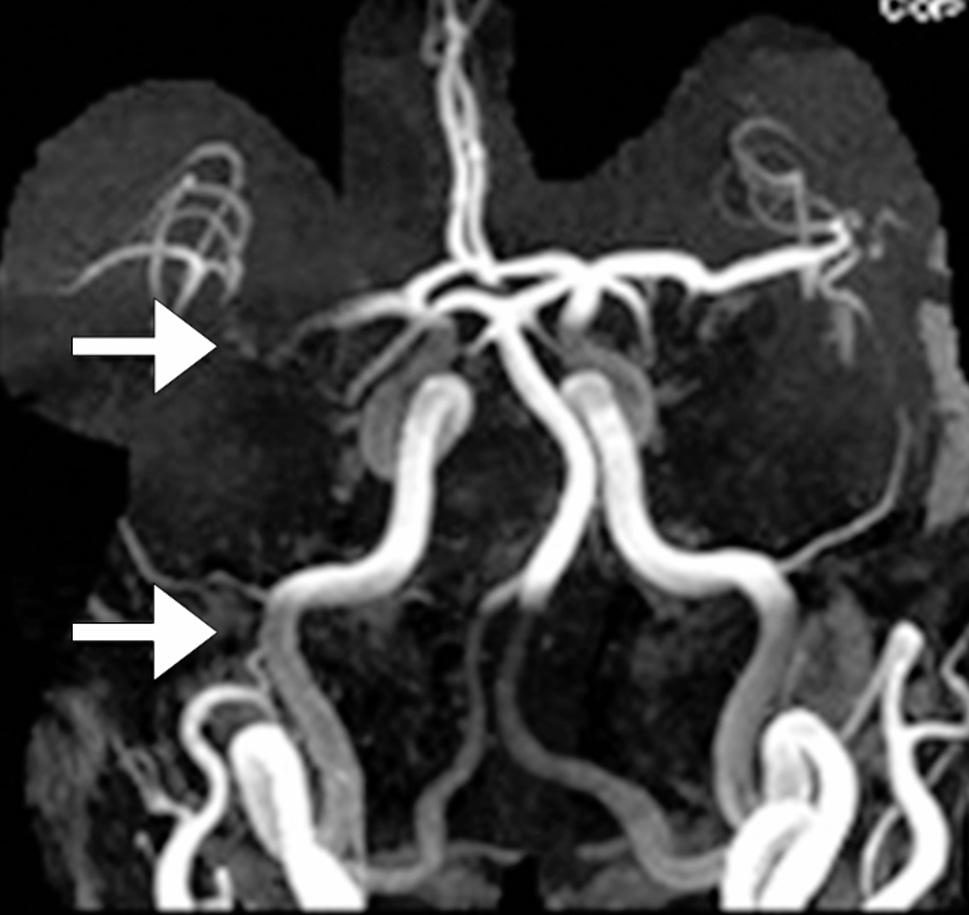
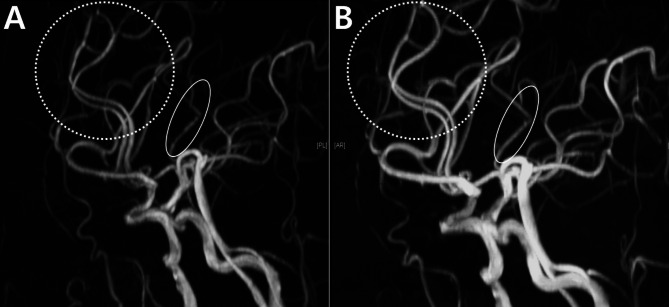
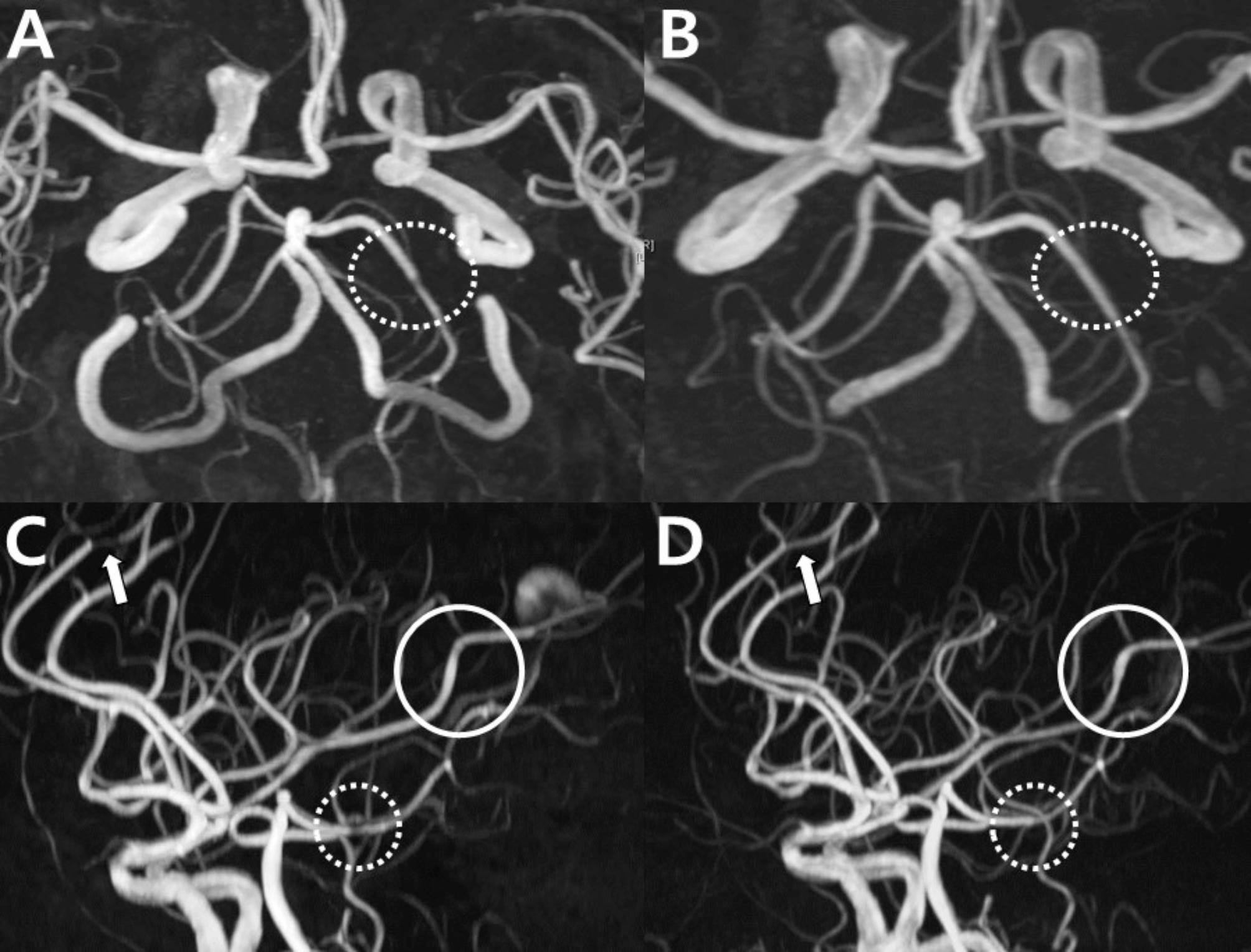
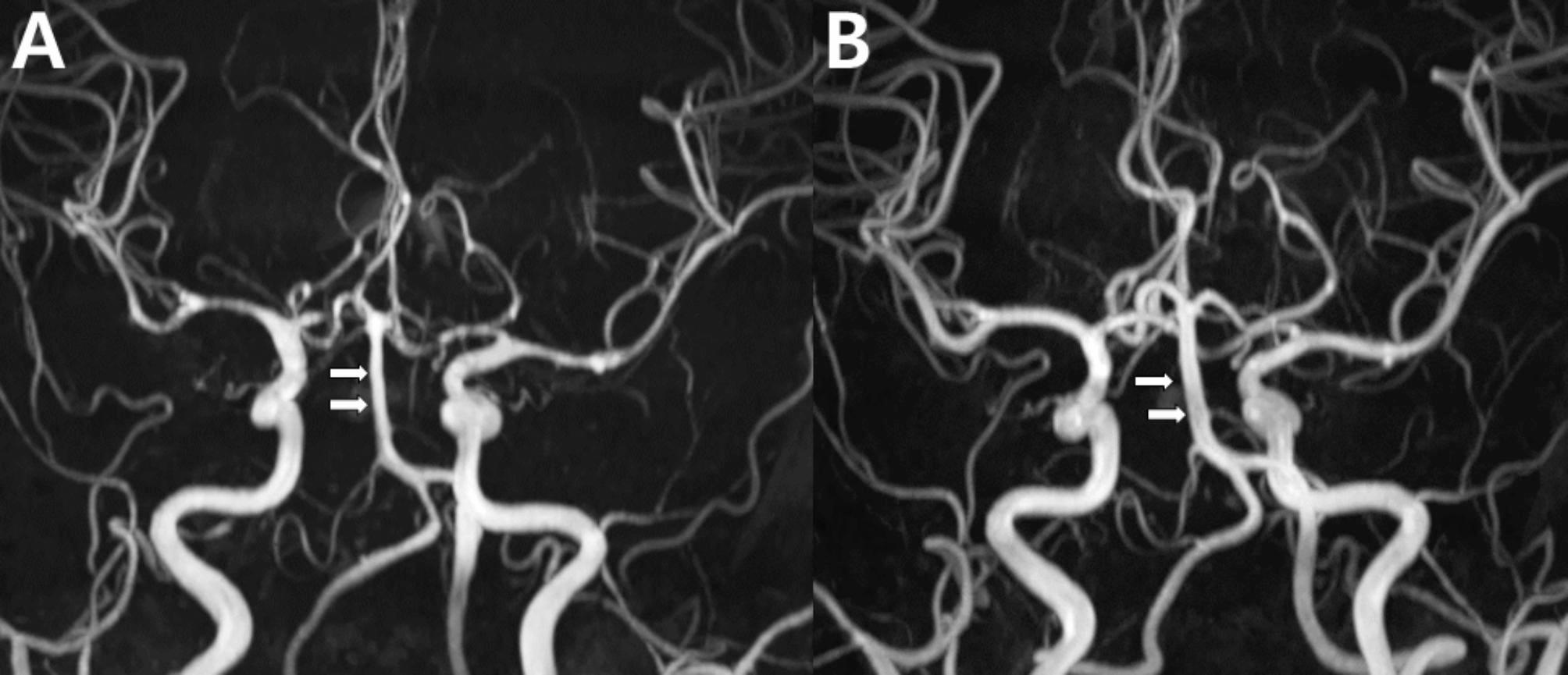
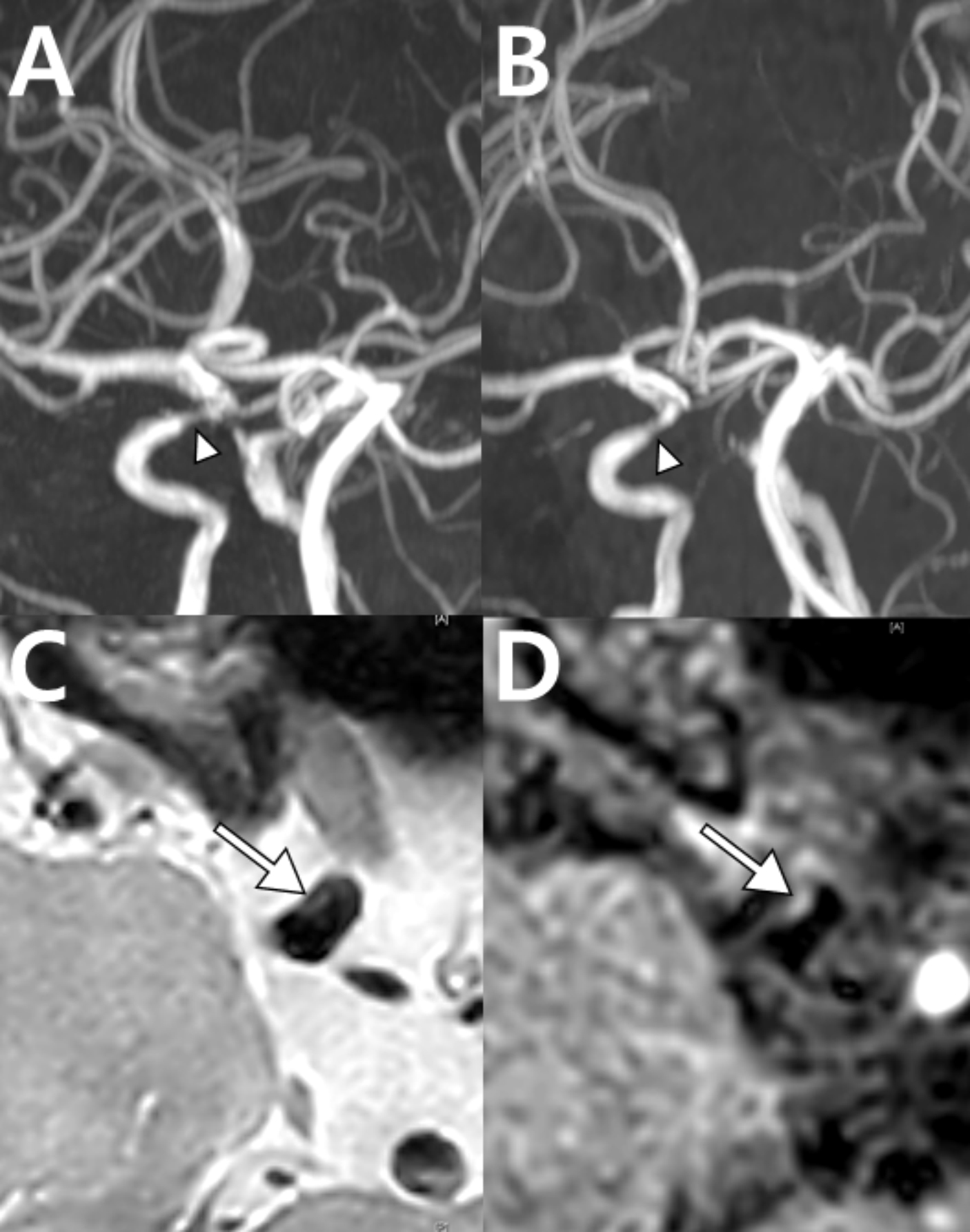
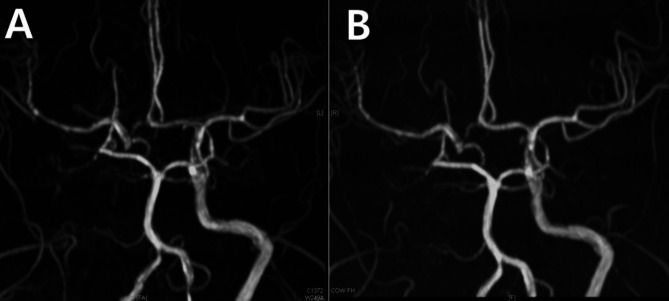
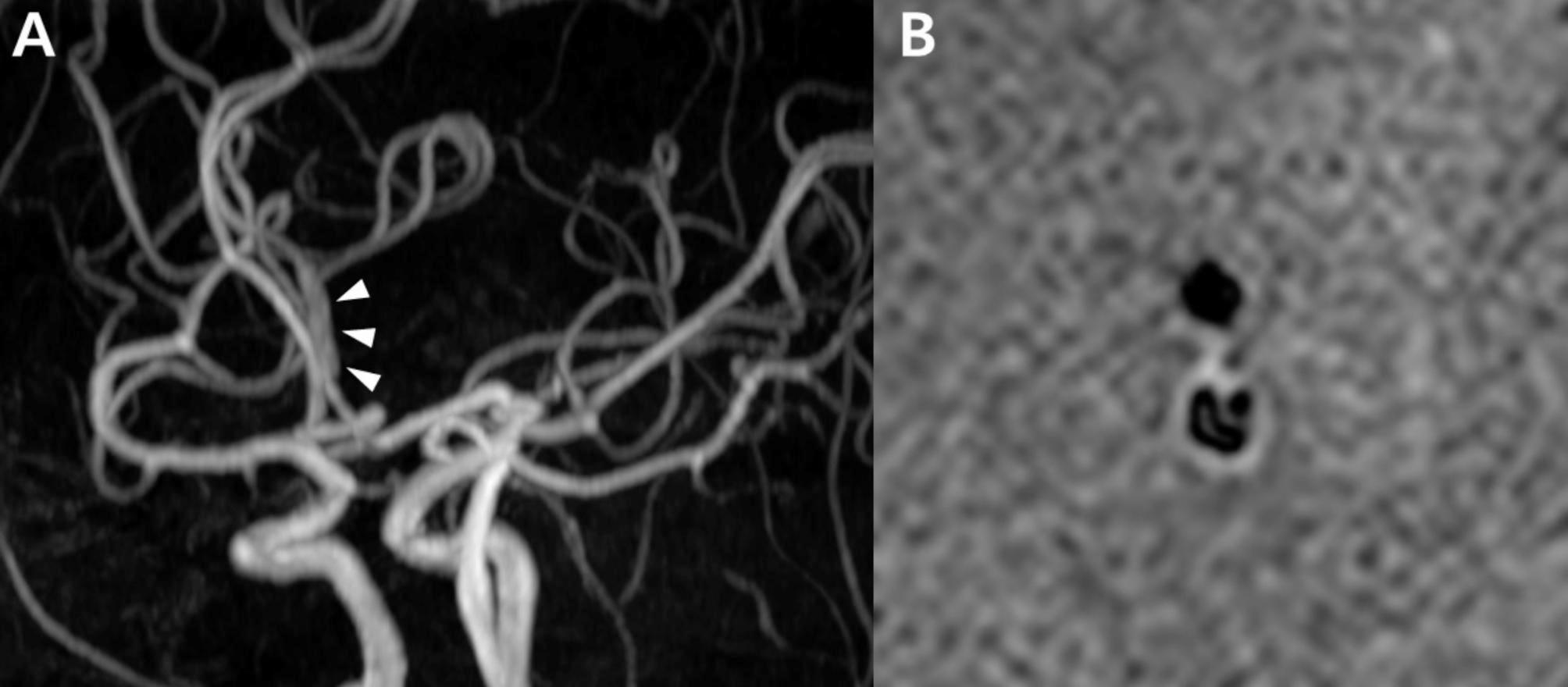
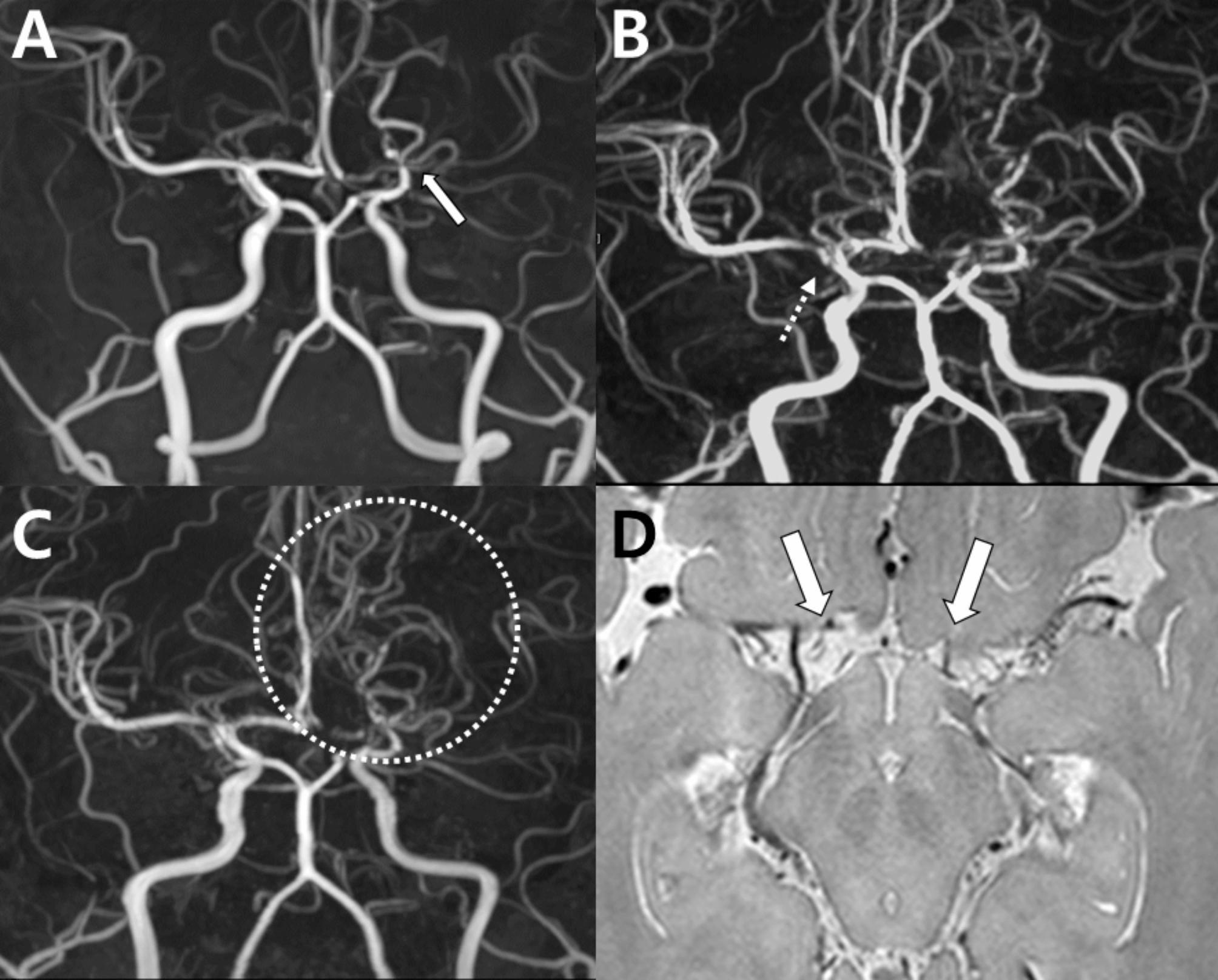
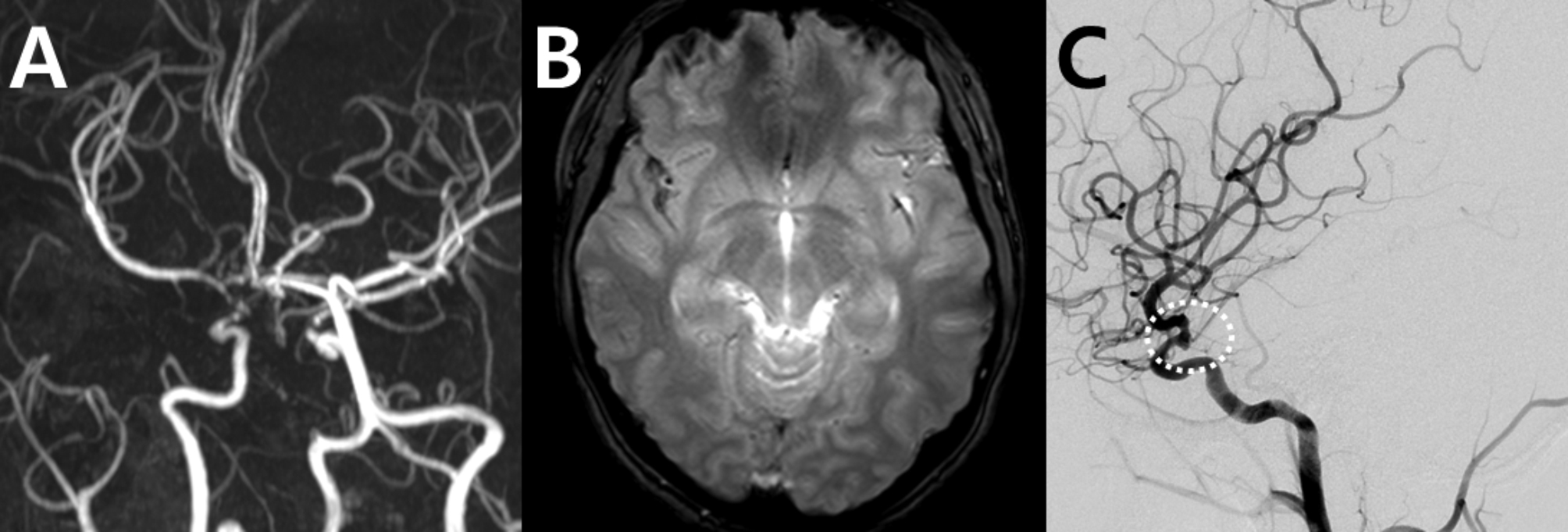
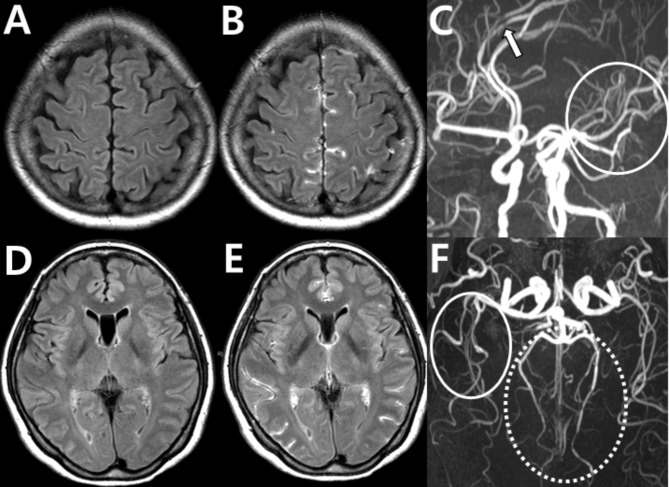
Main body: This review presents a series of cases that show both typical and atypical presentations of RCVS. Typical cases show the characteristic "string of beads" pattern on angiography, which usually resolves within 3-6 months. However, diagnostic challenges arise when angiography appears normal in the early stages or when imaging artifacts obscure the findings. In addition, the variability in vasoconstriction patterns and the need for a differential diagnosis further complicate the accurate identification. These cases highlight the importance of considering RCVS in patients with recurrent thunderclap headaches, even when the initial imaging is inconclusive. Recognizing these challenges and the variability in presentation, along with the use of high-resolution vessel wall MRI and blood-brain barrier imaging, can improve diagnostic accuracy and improve patient outcomes.
Conclusion: The diagnosis of RCVS requires careful integration of clinical evaluation and advanced imaging techniques, with particular attention to radiological findings that can guide accurate diagnosis and management. Despite challenges, such as normal early stage angiography and imaging variability, maintaining a high suspicion of RCVS is essential, especially in patients with recurrent thunderclap headaches.
Keywords: Angiography; Blood-brain barrier imaging; Cerebral vasoconstriction; Differential diagnosis; High-resolution vessel wall MRI; Imaging artifacts; Reversible cerebral vasoconstriction syndrome; Thunderclap headache.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Diffuse cerebral vasodilatation at the initial stage of reversible cerebral vasoconstriction syndrome (RCVS).Rev Neurol (Paris). 2025 Apr;181(4):305-313. doi: 10.1016/j.neurol.2025.01.411. Epub 2025 Feb 26. Rev Neurol (Paris). 2025. PMID: 40016067
-
A case report of reversible cerebral vasoconstriction syndrome with thunderclap headache significantly exacerbated in the supine position and alleviated in the standing position.BMC Neurol. 2023 Oct 3;23(1):348. doi: 10.1186/s12883-023-03381-6. BMC Neurol. 2023. PMID: 37789263 Free PMC article.
-
A common cause of sudden and thunderclap headaches: reversible cerebral vasoconstriction syndrome.J Headache Pain. 2014 Mar 1;15(1):13. doi: 10.1186/1129-2377-15-13. J Headache Pain. 2014. PMID: 24580731 Free PMC article.
-
Reversible cerebral vasoconstriction syndrome: review of neuroimaging findings.Radiol Med. 2022 Sep;127(9):981-990. doi: 10.1007/s11547-022-01532-2. Epub 2022 Aug 6. Radiol Med. 2022. PMID: 35932443 Free PMC article. Review.
-
Narrative Review: Headaches After Reversible Cerebral Vasoconstriction Syndrome.Curr Pain Headache Rep. 2020 Nov 8;24(12):74. doi: 10.1007/s11916-020-00908-1. Curr Pain Headache Rep. 2020. PMID: 33161482 Review.
References
-
- Calabrese LH, Dodick DW, Schwedt TJ, Singhal AB (2007) Narrative review: reversible cerebral vasoconstriction syndromes. Ann Intern Med 146(1):34–44 - PubMed
-
- Ducros A (2012) Reversible cerebral vasoconstriction syndrome. Lancet Neurol 11(10):906–917 - PubMed
-
- Cho SH, Kim BK, Lee MJ (2022) Clinical characteristics of reversible cerebral vasoconstriction syndrome: a large korean multicenter study. Headache Pain Res 23(2):27–32.
-
- Headache Classification Committee of the International Headache Society (IHS) (2018) The International classification of Headache disorders, 3rd edition. Cephalalgia 38(1):1–211 - PubMed
-
- Song TJ, Lee KH, Li H, Kim JY, Chang K, Kim SH, Han KH, Kim BY, Kronbichler A, Ducros A et al (2021) Reversible cerebral vasoconstriction syndrome: a comprehensive systematic review. Eur Rev Med Pharmacol Sci 25(9):3519–3529 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
