

Platelet-to-high-density lipoprotein ratio (PHR) as a predictive biomarker for gastrointestinal cancers: evidence from NHANES
- PMID: 40289098
- PMCID: PMC12036308
- DOI: 10.1186/s12876-025-03860-9
Platelet-to-high-density lipoprotein ratio (PHR) as a predictive biomarker for gastrointestinal cancers: evidence from NHANES
Abstract
Background: Gastrointestinal (GI) cancers, including gastric, colorectal, and esophageal cancers, pose a significant global health burden. Despite advancements in diagnostic tools, early detection remains challenging, particularly in low-resource settings. Emerging evidence highlights the platelet-to-high-density lipoprotein ratio (PHR) as a novel biomarker integrating systemic inflammation and lipid metabolism. However, its association with GI cancer risk remains underexplored.
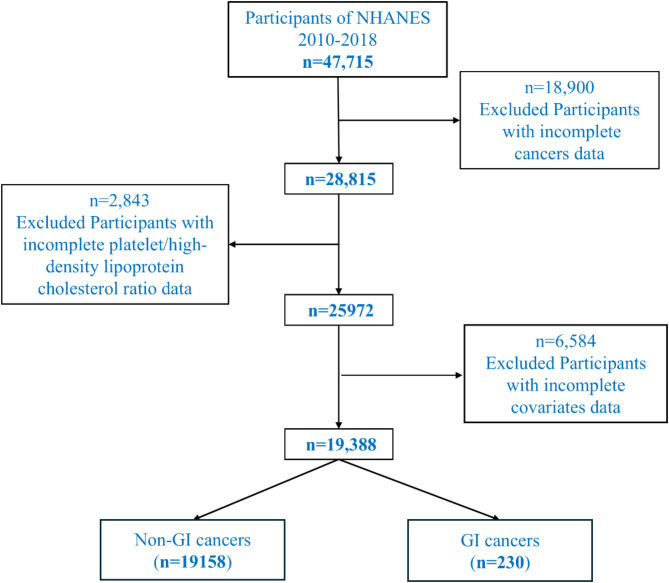
Methods: This study utilized data from the National Health and Nutrition Examination Survey (NHANES) from 2010 to 2018, comprising 19,388 participants, including 230 with GI cancers. PHR was calculated as the ratio of platelet count to high-density lipoprotein cholesterol levels and categorized into quartiles. Weighted logistic regression models, restricted cubic spline analysis, and subgroup analyses were employed to evaluate the association between PHR and GI cancer risk, adjusting for demographic, socioeconomic, lifestyle, and clinical factors.
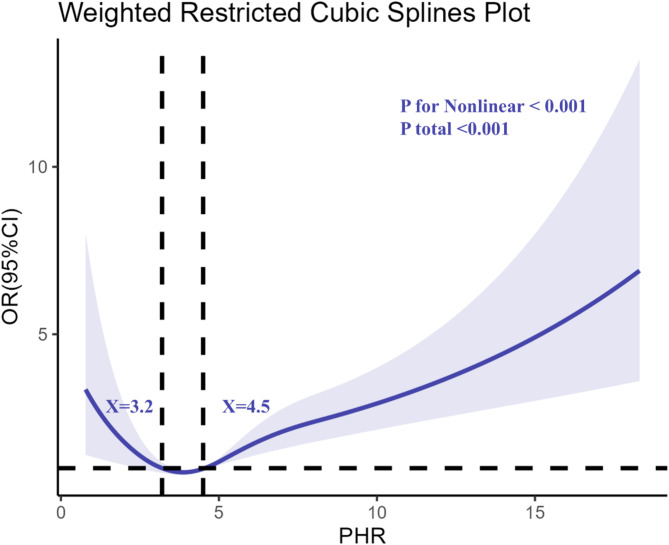
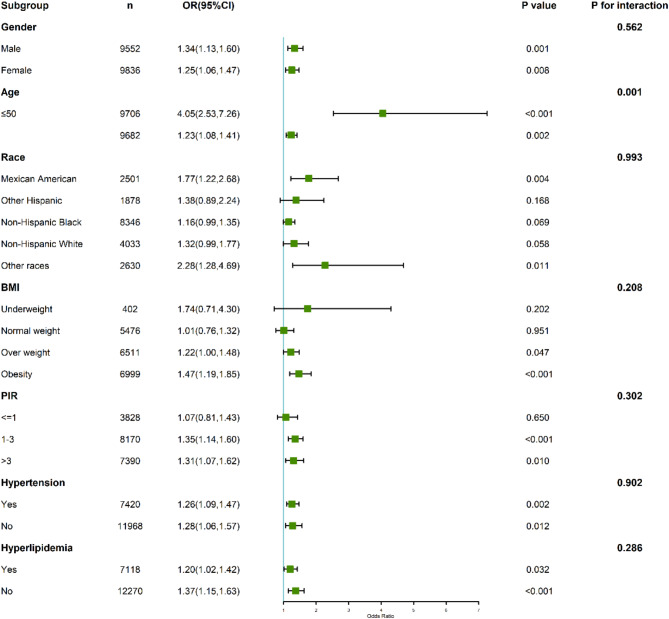
Results: Elevated PHR was independently associated with an increased risk of GI cancers. Participants in the highest PHR quartile exhibited a significantly higher risk (adjusted OR = 3.09; 95% CI: 2.16-4.43) compared to the lowest quartile. A dose-response relationship was observed, with two critical inflection points at PHR values of 3.2 and 4.5. Subgroup analyses revealed stronger associations among older adults, males, and obese individuals. The findings suggest that PHR may reflect the dynamic balance of systemic inflammation and lipid metabolism, contributing to tumorigenesis.
Conclusion: This study identifies PHR as a promising, cost-effective biomarker for early detection and risk stratification of GI cancers. Its integration into screening programs could improve precision medicine strategies by identifying high-risk individuals for early intervention. Further longitudinal and mechanistic studies are warranted to confirm these findings and explore the underlying biological mechanisms.
Keywords: Cancer screening; Dose-response relationship; Gastrointestinal cancers; Lipid metabolism; NHANES; Platelet-to-high-density lipoprotein ratio (PHR).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study utilized publicly available, de-identified data from the National Health and Nutrition Examination Survey (NHANES), which is exempt from additional ethical review according to the National Center for Health Statistics (NCHS) Research Ethics Review Board. No ethical approval was required for this study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Associations of Platelet to High-Density Lipoprotein Cholesterol Ratio with Chronic Obstructive Pulmonary Disease: A Cross-Sectional Study from the US National Health and Nutrition Examination Survey.Int J Chron Obstruct Pulmon Dis. 2024 Oct 23;19:2321-2332. doi: 10.2147/COPD.S481197. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39465032 Free PMC article.
-
The value of the platelet/high-density lipoprotein cholesterol ratio in predicting depression and its cardiovascular disease mortality: a population-based observational study.Front Endocrinol (Lausanne). 2024 Jul 29;15:1402336. doi: 10.3389/fendo.2024.1402336. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39149124 Free PMC article.
-
Platelet to high density lipoprotein cholesterol ratio is associated with diabetes and prediabetes in NHANES 2005 to 2018.Sci Rep. 2024 Dec 3;14(1):30082. doi: 10.1038/s41598-024-81637-y. Sci Rep. 2024. PMID: 39627414 Free PMC article.
-
Identifying Novel Biomarkers Ready for Evaluation in Low-Prevalence Populations for the Early Detection of Upper Gastrointestinal Cancers: A Systematic Review.Adv Ther. 2021 Feb;38(2):793-834. doi: 10.1007/s12325-020-01571-z. Epub 2020 Dec 11. Adv Ther. 2021. PMID: 33306189 Free PMC article.
-
Multicancer Detection (MCD) Testing in Gastrointestinal Cancers: An Evolving Tool for Early Diagnosis.Curr Gastroenterol Rep. 2025 Mar 6;27(1):19. doi: 10.1007/s11894-025-00970-y. Curr Gastroenterol Rep. 2025. PMID: 40047994 Free PMC article. Review.
References
-
- Danpanichkul P, Auttapracha T, Sukphutanan B, Ng CH, Wattanachayakul P, Kongarin S, Dutta P, Duangsonk K, Thongpiya J, Muthiah MD, Huang DQ, Lui RN, Seko Y, Takahashi H, Noureddin M, Yang JD, Wallace MB, Wijarnpreecha K. The burden of overweight and obesity-associated gastrointestinal cancers in low and lower-middle-income countries: a global burden of disease 2019 analysis. Am J Gastroenterol. 2024;119(6):1177–80. 10.14309/ajg.0000000000002819. Epub 2024 Apr 22. PMID: 38900306. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
