

Impact of Lifestyle Medicine Interventions on the Management of Systemic Hypertension in Primary Care: A Canadian Randomized Controlled Trial
- PMID: 40290303
- PMCID: PMC12032512
- DOI: 10.1177/15598276241242013
Impact of Lifestyle Medicine Interventions on the Management of Systemic Hypertension in Primary Care: A Canadian Randomized Controlled Trial
Abstract
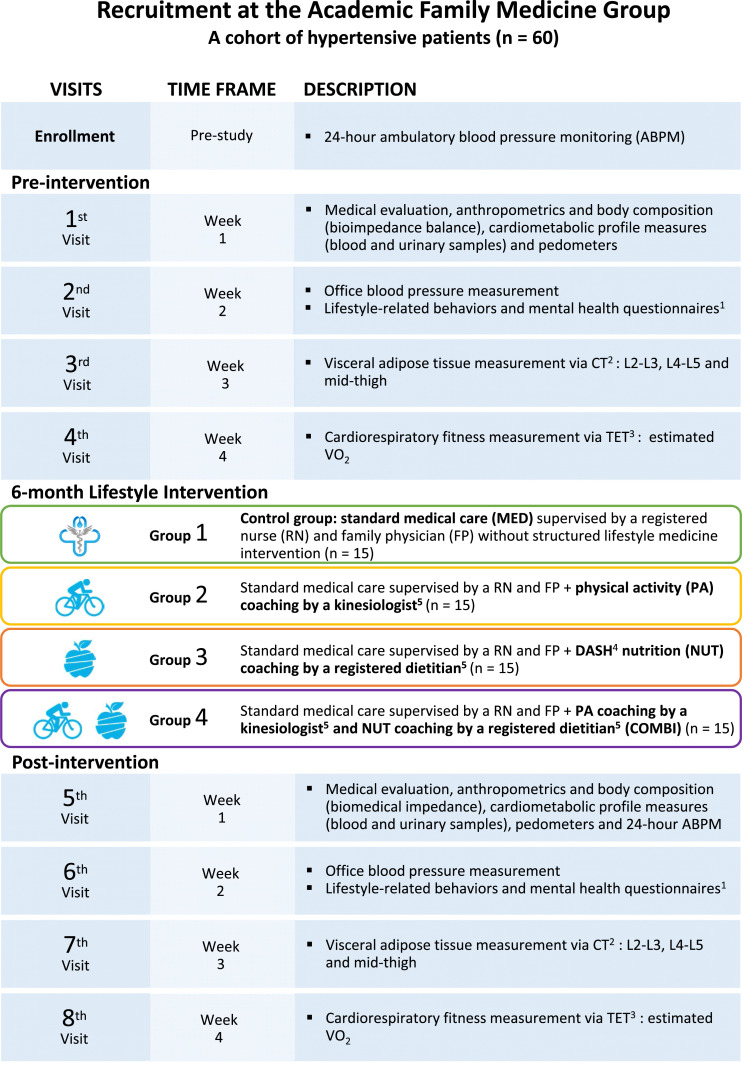
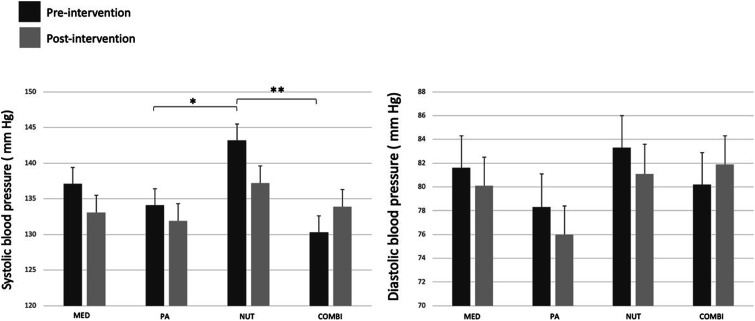
The study aimed to evaluate the feasibility of implementing lifestyle interventions in primary care settings with hypertensive patients and their effect on blood pressure, body composition, cardiometabolic markers, and antihypertensive drug use. Sixty participants diagnosed with stage 1 hypertension were randomly assigned to 4 groups: (1) Standard medical care (control), (2) Physical activity protocol, (3) Dietary Approach to Stop Hypertension (DASH) diet, and (4) Combination of physical activity protocol and DASH diet. Participants received counseling from family physicians, nurses, kinesiologists, and registered dietitians. Various assessments were conducted before (T0) and after (T6) the interventions, including 24-h ambulatory blood pressure monitoring, blood and urine tests, anthropometric measurements, computed tomography to measure adipose tissue, submaximal exercise test to estimate maximal oxygen consumption and health questionnaires. Fifty-one (51) participants (51/57, 89%) completed the program. All interventions reduced blood pressure indices between T0 and T6, except the combined interventions group. Body composition and cardiometabolic parameters were improved in all groups, except for the control group. In total, 28% of participants (7/23) reduced or stopped their antihypertensive medications at T6. The results suggest that structured lifestyle interventions are feasible in primary care and improve blood pressure and cardiometabolic parameters in patients with stage 1 hypertension.
Keywords: hypertension; lifestyle medicine; medication; primary care.
Copyright © 2024 The Author(s).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


Similar articles
-
Technologies for Innovative Monitoring to Reduce Blood Pressure and Change Lifestyle Using Mobile Phones in Adult and Elderly Populations (TIM Study): Protocol for a Randomized Controlled Trial.JMIR Res Protoc. 2018 Aug 7;7(8):e169. doi: 10.2196/resprot.9619. JMIR Res Protoc. 2018. PMID: 30087093 Free PMC article.
-
Effects of a Japanese Cuisine-Based Antihypertensive Diet and Fish Oil on Blood Pressure and Its Variability in Participants with Untreated Normal High Blood Pressure or Stage I Hypertension: A Feasibility Randomized Controlled Study.J Atheroscler Thromb. 2022 Feb 1;29(2):152-173. doi: 10.5551/jat.57802. Epub 2020 Dec 9. J Atheroscler Thromb. 2022. PMID: 33298663 Free PMC article. Clinical Trial.
-
Effects of DASH diet with or without time-restricted eating in the management of stage 1 primary hypertension: a randomized controlled trial.Nutr J. 2024 Jun 17;23(1):65. doi: 10.1186/s12937-024-00967-9. Nutr J. 2024. PMID: 38886740 Free PMC article. Clinical Trial.
-
The 2010 Canadian Hypertension Education Program recommendations for the management of hypertension: part 2 - therapy.Can J Cardiol. 2010 May;26(5):249-58. doi: 10.1016/s0828-282x(10)70379-2. Can J Cardiol. 2010. PMID: 20485689 Free PMC article. Review.
-
The 2007 Canadian Hypertension Education Program recommendations for the management of hypertension: part 2 - therapy.Can J Cardiol. 2007 May 15;23(7):539-50. doi: 10.1016/s0828-282x(07)70798-5. Can J Cardiol. 2007. PMID: 17534460 Free PMC article.
Cited by
-
Effectiveness of a Structured 2-Year Diabetes Health Education Program of Patients with Type 2 Diabetes Mellitus in Disease-Related Serum Markers.Diabetes Metab Syndr Obes. 2025 Jun 4;18:1849-1858. doi: 10.2147/DMSO.S519747. eCollection 2025. Diabetes Metab Syndr Obes. 2025. PMID: 40485872 Free PMC article.
References
-
- Leung AA, Bushnik T, Hennessy D, McAlister FA, Manuel DG. Risk factors for hypertension in Canada. Health Rep. 2019;30(2):3-13. - PubMed
LinkOut - more resources
Full Text Sources