

Aberrant preparation of hand movement in schizophrenia spectrum disorder: an fMRI study
- PMID: 40290422
- PMCID: PMC12022610
- DOI: 10.1093/braincomms/fcaf148
Aberrant preparation of hand movement in schizophrenia spectrum disorder: an fMRI study
Abstract
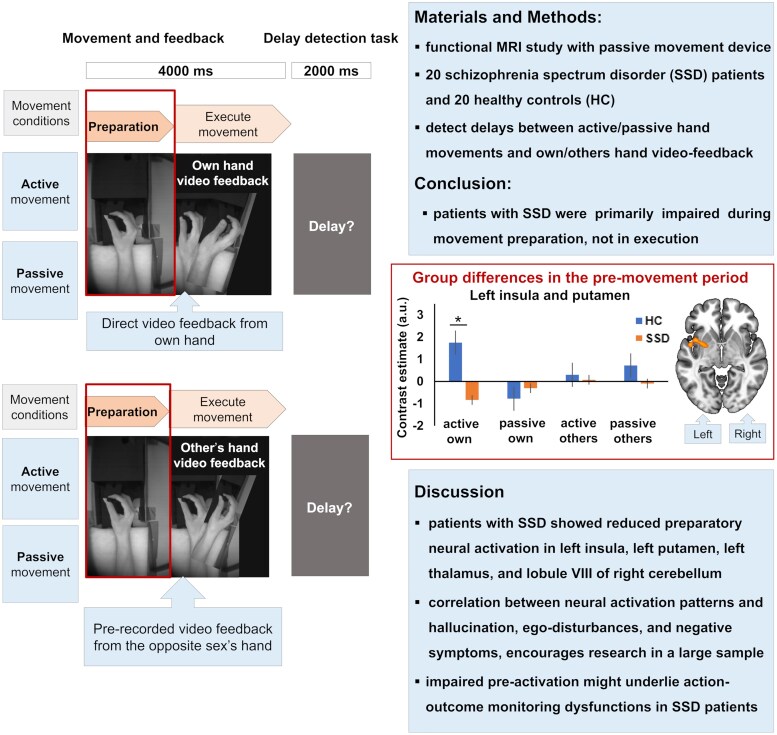
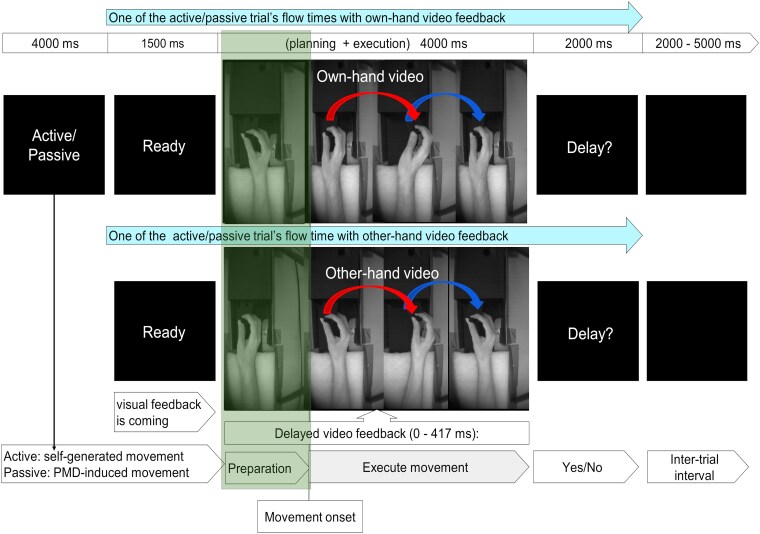
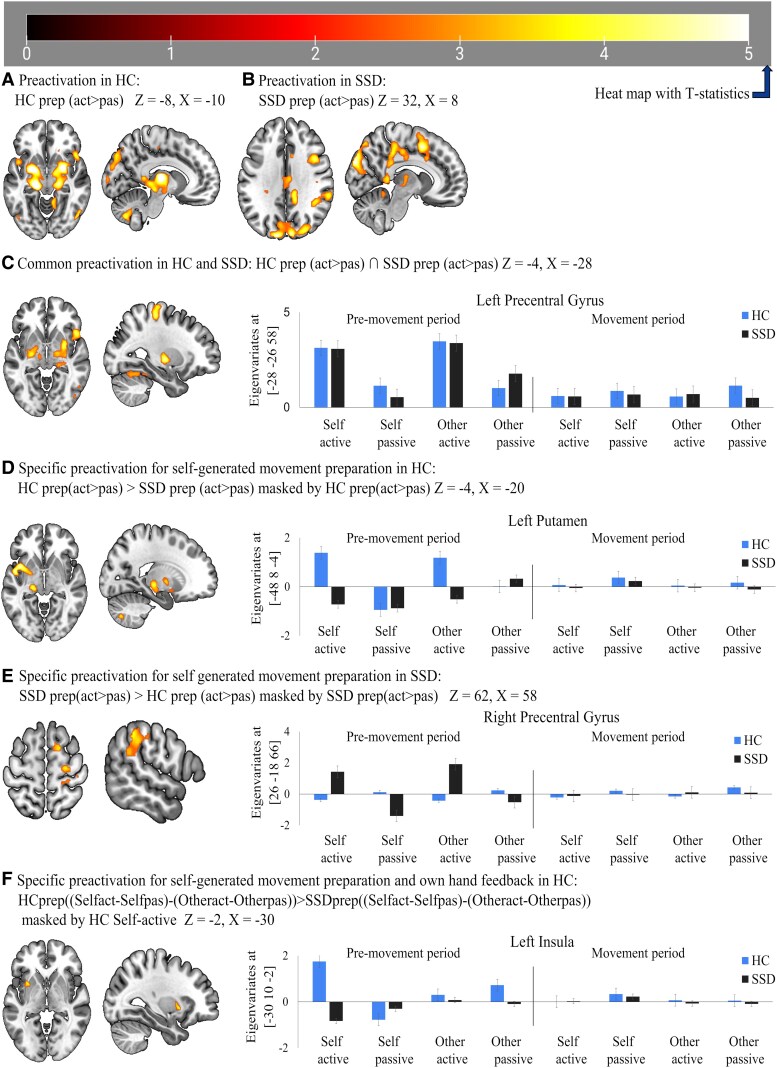
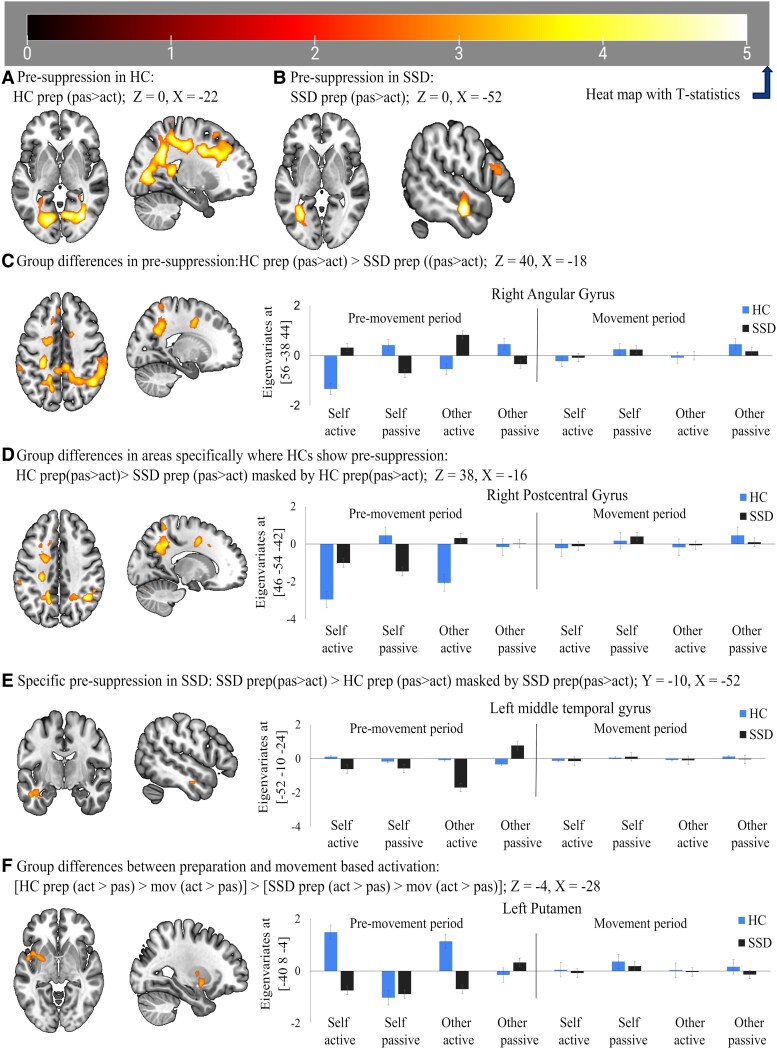
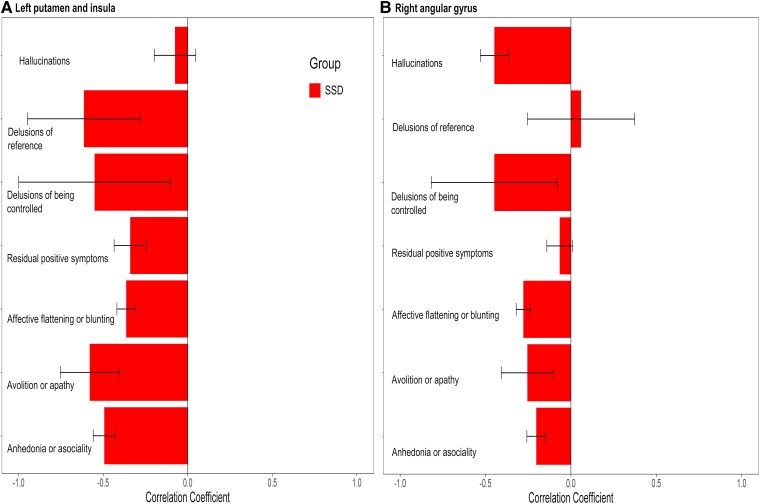
Schizophrenia spectrum disorder is linked to impaired self-other distinction and action feedback monitoring, largely stemming from sensory-motor predictive mechanisms. However, the neural correlates of these predictive processes during movement preparation are unknown. Here, we investigated whether patients with schizophrenia spectrum disorder exhibit aberrant sensory-motor predictive processes reflected in neural activation patterns prior to hand movement onset. Functional MRI data from patients with schizophrenia spectrum disorder (n = 20) and healthy controls (n = 20) were acquired during actively performed or passively induced hand movements. The task required participants to detect temporal delays between their movements and video feedback, which either displayed their own (self) or someone else's (other) hand moving in accordance with their own hand movements. Patients compared with healthy controls showed reduced preparatory blood-oxygen-level-dependent activation (active > passive) in clusters comprising the left putamen, left insula, left thalamus and lobule VIII of the right cerebellum. Reduced activation in the left insula and putamen was specific to own-hand feedback. Additionally, patients with schizophrenia spectrum disorder revealed reduced suppression (passive > active) in bilateral and medial parietal (including the right angular gyrus) and occipital areas, the right postcentral gyrus, cerebellum crus I, as well as the left medial superior frontal gyrus. Ego-disturbances were negatively correlated with left insula and putamen activation during active conditions and with right angular gyrus activation patterns during passive conditions when own-hand feedback was presented. These functional MRI findings suggest that group differences are primarily evident during preparatory processes. Our results show that this preparatory neural activation is further linked to symptom severity, supporting the idea that the preparation of upcoming events as internal predictive mechanisms may underlie severe symptoms in patients with schizophrenia spectrum disorder. These findings could improve our understanding of deficits in action planning, self-monitoring and motor dysfunction in various psychiatric, neurological and neurodegenerative disorders.
Keywords: action-awareness; ego-disturbances; passivity-symptoms; pre-activation; self-other-distinction.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no competing interests.
Figures
Similar articles
-
Temporal characteristics of hemodynamic responses during active and passive hand movements in schizophrenia spectrum disorder.Schizophrenia (Heidelb). 2025 Aug 6;11(1):109. doi: 10.1038/s41537-025-00654-6. Schizophrenia (Heidelb). 2025. PMID: 40770189 Free PMC article.
-
Neural Correlates of Self-other Distinction in Patients with Schizophrenia Spectrum Disorders: The Roles of Agency and Hand Identity.Schizophr Bull. 2021 Aug 21;47(5):1399-1408. doi: 10.1093/schbul/sbaa186. Schizophr Bull. 2021. PMID: 33433625 Free PMC article.
-
Seeing your own or someone else's hand moving in accordance with your action: The neural interaction of agency and hand identity.Hum Brain Mapp. 2020 Jun 15;41(9):2474-2489. doi: 10.1002/hbm.24958. Epub 2020 Feb 24. Hum Brain Mapp. 2020. PMID: 32090439 Free PMC article.
-
Predictive neural processing of self-generated hand and tool actions in patients with schizophrenia spectrum disorders and healthy individuals.Transl Psychiatry. 2025 Mar 17;15(1):85. doi: 10.1038/s41398-025-03306-6. Transl Psychiatry. 2025. PMID: 40097402 Free PMC article.
-
Common and distinct patterns of intrinsic brain activity alterations in major depression and bipolar disorder: voxel-based meta-analysis.Transl Psychiatry. 2020 Oct 19;10(1):353. doi: 10.1038/s41398-020-01036-5. Transl Psychiatry. 2020. PMID: 33077728 Free PMC article. Review.
Cited by
-
Temporal characteristics of hemodynamic responses during active and passive hand movements in schizophrenia spectrum disorder.Schizophrenia (Heidelb). 2025 Aug 6;11(1):109. doi: 10.1038/s41537-025-00654-6. Schizophrenia (Heidelb). 2025. PMID: 40770189 Free PMC article.
References
LinkOut - more resources
Full Text Sources