

A Paradigm for Optimal Management: Traumatic Neck Injuries at a Tertiary Care Centre in South India
- PMID: 40291240
- PMCID: PMC12033068
- DOI: 10.7759/cureus.81311
A Paradigm for Optimal Management: Traumatic Neck Injuries at a Tertiary Care Centre in South India
Abstract
Introduction: Traumatic neck injuries represent a critical emergency in surgical practice due to the high concentration of vital structures within the cervical region. These injuries can be classified into blunt and penetrating types, each presenting unique challenges in diagnosis and management. While advances in trauma care have improved patient outcomes, the mortality and morbidity associated with neck injuries remain significant, especially in resource-limited settings.
Materials and methods: A retrospective cohort study was conducted at Government Medical College, Thrissur, analyzing the patterns, management, and outcomes of traumatic neck injuries from January 2022 to December 2024. The study included patients aged 13-79 years, with data collected from medical records, trauma registers, and operative reports. Patient demographics, injury type, anatomical location, management strategies, and clinical outcomes were assessed.
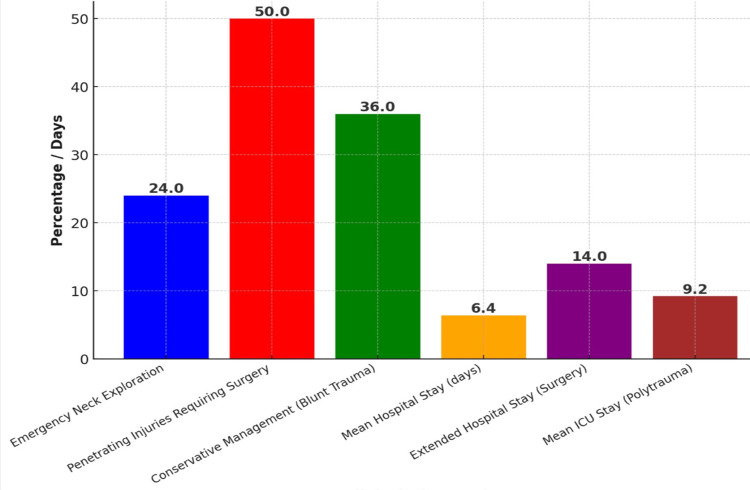
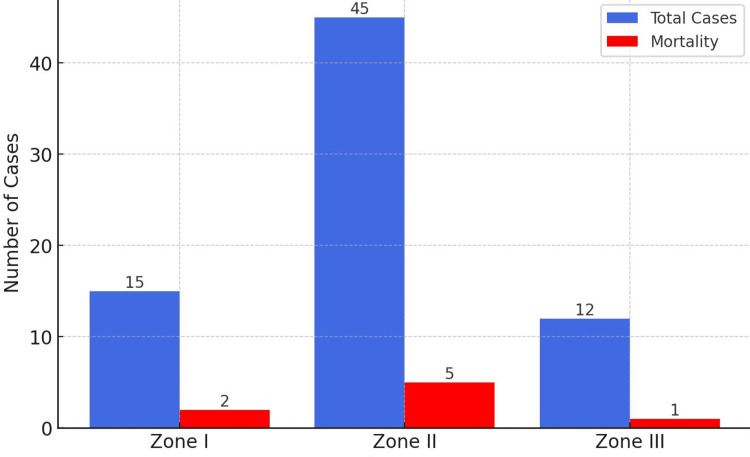
Results: A total of 72 traumatic neck injuries were reviewed, with the majority being young males (n=57, 79%). Blunt trauma (n=45, 62%) was more common than penetrating trauma (n=27, 38%), with road traffic accidents (n=32, 44%) and falls (n=20, 28%) being the leading causes of blunt injuries, while stabbing injuries accounted for most penetrating trauma (n=20, 73%). Emergency neck exploration was required in 17 cases (24%), and the overall mortality rate was seven cases (10%), primarily due to exsanguination (n=5, 67%) and vascular damage (n=2, 33%). The highest mortality was observed in penetrating Zone II injuries (n=5 deaths, 13%), often involving major vascular damage. Complications occurred in 13 survivors (18%), including wound infections (n=6, 8%), pneumonia (n=4, 5%), and neurological deficits (n=4, 5%). Night-time injuries were reported in 43 cases (60%), with a peak incidence during festive seasons and weekends, showing a significant association with alcohol consumption.
Discussion: The findings align with global trends, where penetrating injuries, especially in Zone II, carry a significantly higher risk of mortality. The study underscores the importance of early airway management, rapid surgical intervention, and the role of imaging-based triage for blunt trauma cases. The association of neck trauma with alcohol consumption, especially during nighttime hours, highlights the need for targeted public health measures and enhanced trauma response.
Conclusion: This study provides valuable insights into the epidemiology, management strategies, and outcomes of traumatic neck injuries in a South Indian tertiary care center. The findings emphasize the critical role of early intervention, particularly in penetrating injuries involving vascular structures, and suggest that public health interventions and improved trauma care systems could optimize outcomes in this high-risk population.
Keywords: general trauma surgery; neck vascular injury; penetrating injuries; road traffic injuries; stab injury.
Copyright © 2025, Chirukandath et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Ethics Committee, Government Medical College, Thrissur issued approval IEC/GMCTSR/2024/235. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- 5-year management and outcomes of penetrating neck injury in a trauma center. Reyna-Sepúlveda F, Cantu-Alejo D, Martinez-Fernandez A, et al. Cir Esp (Engl Ed) 2022;100:629–634. - PubMed
-
- Management of penetrating neck injuries: a new paradigm for civilian trauma. Bell RB, Osborn T, Dierks EJ, Potter BE, Long WB. J Oral Maxillofac Surg. 2007;65:691–705. - PubMed
-
- Pediatric penetrating neck trauma: hard signs of injury and selective neck exploration. Tessler RA, Nguyen H, Newton C, Betts J. J Trauma Acute Care Surg. 2017;82:989–994. - PubMed
-
- Selective management of penetrating neck injuries using "no zone" approach. Prichayudh S, Choadrachata-anun J, Sriussadaporn S, Pak-art R, Sriussadaporn S, Kritayakirana K, Samorn P. Injury. 2015;46:1720–1725. - PubMed
LinkOut - more resources
Full Text Sources