

Optimizing Anticoagulation Strategies in Patients With Atrial Fibrillation and Valvular Heart Disease: A Comprehensive Evidence-Based Review
- PMID: 40291263
- PMCID: PMC12033385
- DOI: 10.7759/cureus.81319
Optimizing Anticoagulation Strategies in Patients With Atrial Fibrillation and Valvular Heart Disease: A Comprehensive Evidence-Based Review
Abstract
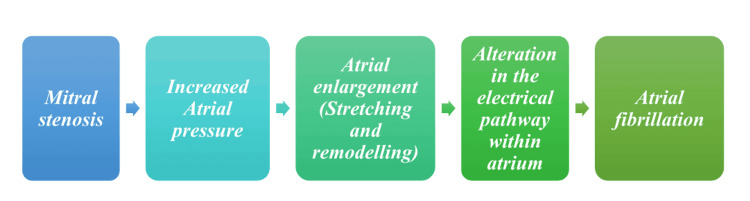
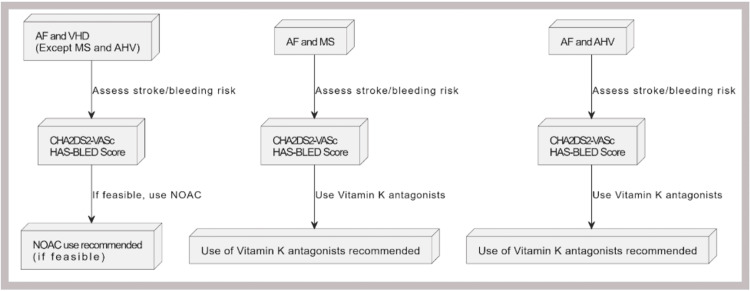
Atrial fibrillation (AF), the most common sustained cardiac arrhythmia, significantly increases the risk of thromboembolism and stroke. Its coexistence with valvular heart disease (VHD) further complicates management due to elevated risks of thromboembolism, bleeding, and mortality. This review explores the pathophysiology of AF and its interaction with VHD, focusing on diagnostic tools like echocardiography and risk stratification scores such as CHA2DS2-VASc and HAS-BLED. Vitamin K antagonists (VKAs) remain the cornerstone of anticoagulation therapy in high-risk VHD populations, particularly in patients with mechanical heart valves or moderate-to-severe mitral stenosis (MS). VKAs have demonstrated proven efficacy in reducing thromboembolic events in these subgroups, supported by decades of clinical evidence. However, their use requires frequent international normalized ratio (INR) monitoring and is associated with higher bleeding risks, posing challenges in long-term management. Despite these limitations, VKAs are indispensable in these populations due to the lack of robust evidence supporting the safety and efficacy of direct oral anticoagulants (DOACs) in these high-risk groups. Ongoing clinical trials, such as the RIVER trial, aim to evaluate the role of DOACs in VHD. However, current guidelines continue to recommend VKAs as the standard of care for these patients. In contrast, DOACs offer significant advantages in non-valvular AF and selected VHD populations. Their predictable pharmacokinetics, fewer dietary restrictions, and lower risks of intracranial hemorrhage make them a preferred choice for many patients. Landmark trials and meta-analyses, including RE-LY, ROCKET-AF, and ARISTOTLE, have demonstrated the safety and efficacy of DOACs in non-valvular AF and certain VHD subgroups. However, DOACs are contraindicated in high-risk VHD populations, such as those with mechanical valves or moderate-to-severe MS, due to insufficient evidence and potential risks of thromboembolic events. Evolving guidelines from leading societies emphasize individualized approaches and collaborative decision-making in anticoagulation therapy. While DOACs are preferred for most AF patients, VKAs remain essential for high-risk VHD patients. Future advancements, such as factor XIa inhibitors, hold promise for improving outcomes and safety in these complex populations. This review provides a comprehensive framework for clinicians to navigate the complexities of anticoagulation in AF and VHD, ensuring evidence-based, patient-centered care.
Keywords: atrial fibrillation (af); direct acting oral anticoagulant; echocardiography; heart failure; international normalized ratio (inr); low-molecular weight heparin; mitral stenosis (ms); rivaroxaban dosing; valvular heart disease; warfarin.
Copyright © 2025, Deiveegan et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Anticoagulation, atherosclerosis, and heart failure. Agewall S. Eur Heart J Cardiovasc Pharmacother. 2017;3:1–2. - PubMed
-
- Anticoagulation therapy in heart failure and sinus rhythm: a systematic review and meta-analysis. Beggs SA, Rørth R, Gardner RS, McMurray JJ. Heart. 2019;105:1325–1334. - PubMed
-
- Anticoagulation in atrial fibrillation with heart failure. Zhao L, Wang WY, Yang X. Heart Fail Rev. 2018;23:563–571. - PubMed
Publication types
LinkOut - more resources
Full Text Sources