

Comparative Analysis of Adverse Event Profiles Among Seven Statins for Hypercholesterolemia Management Using the United States FDA Adverse Event Reporting System
- PMID: 40291284
- PMCID: PMC12032439
- DOI: 10.7759/cureus.81260
Comparative Analysis of Adverse Event Profiles Among Seven Statins for Hypercholesterolemia Management Using the United States FDA Adverse Event Reporting System
Abstract
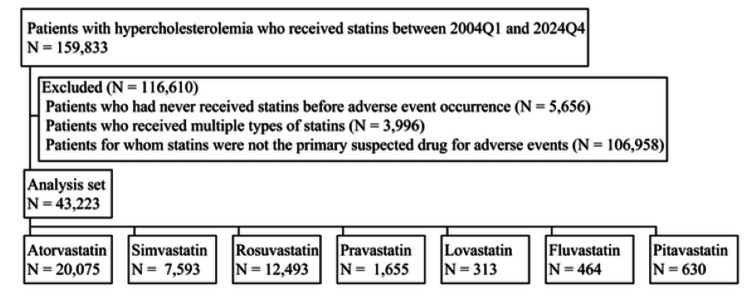
Background Statins are fundamental in hypercholesterolemia management, with seven primary drugs available: atorvastatin, simvastatin, rosuvastatin, pravastatin, lovastatin, fluvastatin, and pitavastatin. While sharing a common mechanism of action, these statins exhibit variations in pharmacokinetic (what the body does to the drug) and pharmacodynamic (what the drug does to the body) properties (e.g., lipophilicity, cytochrome P450 metabolism), which may influence their safety profiles. Adverse events (AEs) such as myopathy and hepatotoxicity vary across agents, complicating clinical decision-making. The guidelines lack robust comparisons of all seven statins' AE profiles, presenting challenges for clinicians in balancing potency and tolerability. Objectives This study aimed to comprehensively compare the AE patterns and safety profiles of the seven statins in hypercholesterolemia management through a retrospective analysis of the United States Food and Drug Administration Adverse Event Reporting System (FAERS) database. By focusing solely on hypercholesterolemia, we aimed to control for potential confounding factors, providing a more focused comparison of statin safety profiles. Methods We conducted a retrospective analysis using data from the FAERS between 2004 and 2024. To control for confounding factors, this study included only patients prescribed statins with a clearly documented indication of hypercholesterolemia management. Patients prescribed statins for other indications or with missing data on the reason for prescription were excluded. Comparative evaluations employed the reporting odds ratio (ROR) and adjusted ROR (aROR), which were chosen for their efficiency in ease of interpretation, ability to adjust for confounding factors, and compatibility with statistical testing frameworks. This compatibility allowed for rigorous multiple comparison analysis, where each statin was sequentially set as a reference in 21 pairwise comparisons. To address the multiple comparisons problem, this study applied the Bonferroni correction, adjusting the significance level to 0.05 / 21 = 0.0024. Patient background variables were used as adjustment factors for the aROR. AEs were classified into 10 categories based on their characteristics. Results With atorvastatin as the reference, five statins (simvastatin, rosuvastatin, pravastatin, fluvastatin, and pitavastatin) demonstrated both significant ROR > 1 and aROR > 1 for gastrointestinal disorders. Conversely, five statins (simvastatin, rosuvastatin, pravastatin, lovastatin, and pitavastatin) demonstrated both significant ROR < 1 and aROR < 1 for metabolic disorders. When other statins were set as the reference, no consistent pattern of exclusively significant ROR > 1 and aROR > 1 or significant ROR < 1 and aROR < 1 was observed across all AE categories. Instead, a heterogeneous distribution of outcomes was evident. These results indicate that the patterns of AEs differ for each statin. Conclusions This study reveals distinct AE profiles among seven statins, providing critical insights to guide personalized treatment strategies. By aligning patient risk factors with specific statin AE profiles, clinicians can implement more targeted approaches to minimize AEs, potentially improving adherence and treatment efficacy. These findings directly inform clinical decision-making, enabling healthcare providers to optimize statin selection and management for individual patients.
Keywords: cardiovascular risk; database; drug safety; multiple comparisons; personalized medicine; pharmacoepidemiology.
Copyright © 2025, Ogura et al.
Conflict of interest statement
Human subjects: All authors have confirmed that this study did not involve human participants or tissue. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Comparison of Adverse Events Among Angiotensin Receptor Blockers in Hypertension Using the United States Food and Drug Administration Adverse Event Reporting System.Cureus. 2025 Apr 8;17(4):e81912. doi: 10.7759/cureus.81912. eCollection 2025 Apr. Cureus. 2025. PMID: 40342468 Free PMC article.
-
A survey of the FDA's AERS database regarding muscle and tendon adverse events linked to the statin drug class.PLoS One. 2012;7(8):e42866. doi: 10.1371/journal.pone.0042866. Epub 2012 Aug 22. PLoS One. 2012. PMID: 22936996 Free PMC article.
-
Statin-related neurocognitive disorder: a real-world pharmacovigilance study based on the FDA adverse event reporting system.Expert Rev Clin Pharmacol. 2024 Mar;17(3):255-261. doi: 10.1080/17512433.2024.2311875. Epub 2024 Jan 31. Expert Rev Clin Pharmacol. 2024. PMID: 38275183
-
Pharmacokinetic drug-drug interactions between 1,4-dihydropyridine calcium channel blockers and statins: factors determining interaction strength and relevant clinical risk management.Ther Clin Risk Manag. 2014;10:17-26. doi: 10.2147/TCRM.S55512. Epub 2013 Dec 20. Ther Clin Risk Manag. 2014. PMID: 24379677 Free PMC article. Review.
-
Chemical, pharmacokinetic and pharmacodynamic properties of statins: an update.Fundam Clin Pharmacol. 2005 Feb;19(1):117-25. doi: 10.1111/j.1472-8206.2004.00299.x. Fundam Clin Pharmacol. 2005. PMID: 15660968 Review.
Cited by
-
Comparison of Adverse Events Among Angiotensin Receptor Blockers in Hypertension Using the United States Food and Drug Administration Adverse Event Reporting System.Cureus. 2025 Apr 8;17(4):e81912. doi: 10.7759/cureus.81912. eCollection 2025 Apr. Cureus. 2025. PMID: 40342468 Free PMC article.
References
-
- Structural mechanism for statin inhibition of HMG-CoA reductase. Istvan ES, Deisenhofer J. Science. 2001;292:1160–1164. - PubMed
-
- 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Mach F, Baigent C, Catapano AL, et al. Eur Heart J. 2020;41:111–188. - PubMed
-
- Chemical, pharmacokinetic and pharmacodynamic properties of statins: an update. Schachter M. Fundam Clin Pharmacol. 2005;19:117–125. - PubMed
LinkOut - more resources
Full Text Sources