

A Case-Based Approach to the Management of Corneal Melts and Perforations in Ocular Surface Disorders
- PMID: 40291310
- PMCID: PMC12033023
- DOI: 10.7759/cureus.81293
A Case-Based Approach to the Management of Corneal Melts and Perforations in Ocular Surface Disorders
Abstract
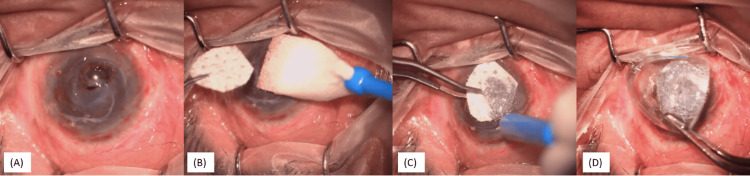
Corneal perforations caused by chronic ocular surface disorders present significant management challenges and can lead to blindness if untreated. This case series reviews the pathophysiology of corneal melts and examines treatment strategies tailored to the size, location, and etiology of perforations in conditions such as Stevens-Johnson syndrome, graft-versus-host disease, and chemical injuries. Through detailed case analyses, various interventions, including cyanoacrylate glue, Tenon's patch grafting, mucous membrane grafts, scleral patch grafts, and conjunctival flaps, were evaluated, along with emerging therapies like biosynthetic hydrogels and collagen-like peptides. Findings highlight the role of chronic inflammation and adnexal abnormalities in disrupting ocular surface integrity, affecting treatment outcomes. This case series underscores the importance of a comprehensive approach that not only repairs corneal defects but also addresses underlying systemic and ocular conditions, with advancements in biosynthetic materials showing promise for improving patient outcomes.
Keywords: chronic inflammation; corneal perforation; limbal stem cell deficiency (lscd); ocular surface disorders; visual rehabilitation.
Copyright © 2025, Gour et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures









References
-
- Non-traumatic corneal perforations: aetiology, treatment and outcomes. Loya-Garcia D, Serna-Ojeda JC, Pedro-Aguilar L, Jimenez-Corona A, Olivo-Payne A, Graue-Hernandez EO. Br J Ophthalmol. 2017;101:634–639. - PubMed
-
- Management of corneal perforation. Jhanji V, Young AL, Mehta JS, Sharma N, Agarwal T, Vajpayee RB. Surv Ophthalmol. 2011;56:522–538. - PubMed
-
- Important concepts for treating ocular surface and tear disorders. Tseng SC, Tsubota K. Am J Ophthalmol. 1997;124:825–835. - PubMed
Publication types
LinkOut - more resources
Full Text Sources