

Treatment decision algorithms for tuberculosis screening and diagnosis in children below 5 years hospitalised with severe acute malnutrition: a cost-effectiveness analysis
- PMID: 40291345
- PMCID: PMC12033959
- DOI: 10.1016/j.eclinm.2025.103206
Treatment decision algorithms for tuberculosis screening and diagnosis in children below 5 years hospitalised with severe acute malnutrition: a cost-effectiveness analysis
Abstract
Background: Children with severe acute malnutrition (SAM) are an important risk group for underdiagnosis and death from tuberculosis. In 2022, the World Health Organization (WHO) recommended use of treatment decision algorithms (TDAs) for tuberculosis diagnosis in children. There is currently no cost-effectiveness evidence for TDA-based approaches compared to routine practice.
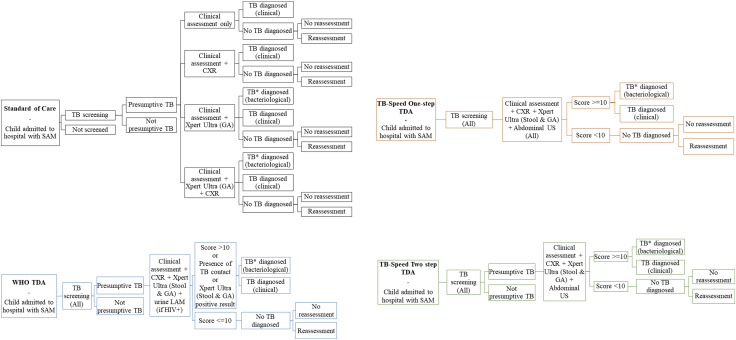
Methods: The TB-Speed SAM study developed i) a one-step TDA including Xpert, clinical, radiological and echography features, and ii) a two-step TDA, which also included a screening phase, for children under 5 years hospitalised with SAM at three tertiary hospitals in Uganda and Zambia from 4th November 2019 to 20th June 2022. This study is registered with ClinicalTrials.gov, NCT04240990. We assessed the diagnostic accuracy and cost-effectiveness of deploying TB-Speed and WHO TDA-based approaches compared to the standard of care (SOC). Estimated outcomes included children started on tuberculosis treatment, false positive rates, disability-adjusted life years (DALYs) and incremental cost-effectiveness ratios (ICERs).
Findings: Per 100 children hospitalised with SAM, averaging 19 children with tuberculosis, the one-step TDA initiated 17 true positive children (95% uncertainty intervals [UI]: 12-23) on tuberculosis treatment, the two-step TDA 15 (95%UI: 10-22), the WHO TDA 14 (95%UI: 9-19), and SOC 4 (95%UI: 2-9). The WHO TDA generated the most false positives (35, 95%UI: 24-46), followed by the one-step TDA (18, 95%UI: 6-29), the two-step TDA (14, 95%UI: 1-25), and SOC (11, 95%UI: 3-17). All TDA-based approaches had ICERs below plausible country cost-effectiveness thresholds compared to SOC (one-step: $44-51/DALY averted, two-step: $34-39/DALY averted, WHO: $40-46/DALY averted).
Interpretation: Our findings show that these TDA-based approaches are highly cost-effective for the vulnerable group of children hospitalised with SAM, compared to current practice.
Funding: Unitaid Grant number: 2017-15-UBx-TB-SPEED.
Keywords: Cost-effectiveness analysis; Diagnosis; Low- and middle-income countries; Paediatric tuberculosis; Severe acute malnutrition; Treatment decision algorithms.
© 2025 The Authors.
Conflict of interest statement
All authors declare no competing interests.
Figures


References
-
- World Health Organization . 2024. Global tuberculosis report. Geneva.
Associated data
LinkOut - more resources
Full Text Sources
Medical
