

[Utilization of apneic oxygenation in anesthesiology: a nationwide survey in Germany]
- PMID: 40293451
- PMCID: PMC12081577
- DOI: 10.1007/s00101-025-01529-2
[Utilization of apneic oxygenation in anesthesiology: a nationwide survey in Germany]
Abstract
Background and research question: While patient safety during general anesthesia has improved in recent years, incidents still occur during anesthesia, particularly in the area of extended airway management. During the induction of general anesthesia, spontaneous breathing is routinely suspended thereby increasing the risk of hypoxemia during the apneic phase. To prevent desaturation and clinically significant hypoxemia, preoxygenation is performed before anesthesia induction. While preoxygenation can extend the safe apnea time, certain high-risk patient groups, such as obese patients, pregnant women, children and those with difficult airways, may require additional stabilization strategies. Apneic oxygenation (ApOx), a technique first described in the early twentieth century, delivers 100% oxygen at a flow rate of 15 l per min or more during the apneic phase to prolong oxygenation. While current airway management guidelines recommend ApOx during the laryngoscopy phase for patients at risk, its widespread utilization in clinical practice remains limited.
Objective: This study presents the findings of a multicenter, web-based survey investigating the use of ApOx in anesthesiology departments across Germany, highlighting the challenges in implementation and identifying areas for further improvement.
Materials and methods: Between 1 July 2024 and 3 September 2024 a multicenter, exploratory, anonymous survey of anesthetists in various German hospitals was conducted. The survey was conducted via the online platform Lime Survey (Hamburg/Germany). Participants were asked about their personal and institutional background and the use of ApOx in their institution The study is based on descriptive statistics.
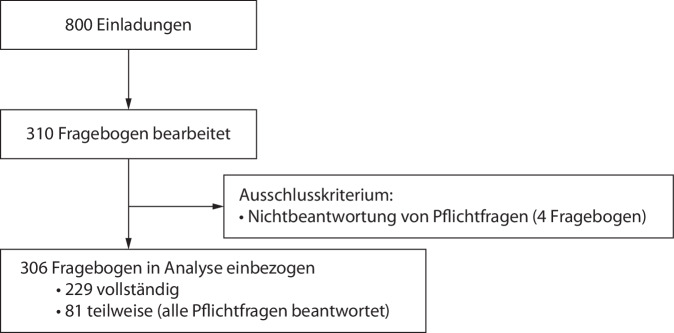
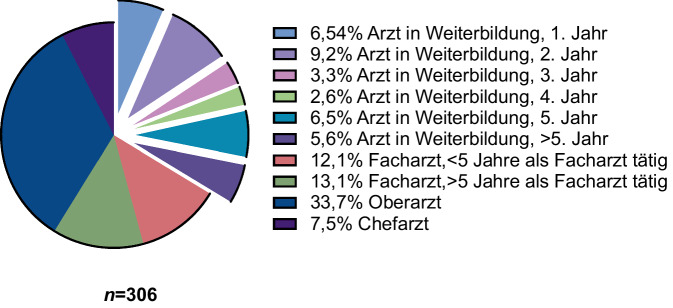
Results: The survey was completed by a total of n = 310 anesthetists and after excluding incomplete data sets, n = 306 questionnaires could be analyzed. The majority of participants were male (63%), with an average age of 41 years (± 10.4). In terms of professional roles, there was an even split between senior physicians (34%) and residents (34%), followed by consultants (25%) or heads of departments (8%). The work settings included university hospitals (37%), maximum care hospitals (27%), intermediate care hospitals (19%) and basic and standard care hospitals (15%). The majority of the participants (59%) had an additional qualification in emergency medicine. In addition, 48% of the respondents had an additional qualification in intensive care medicine. In 84% of cases it was found that neither in-hospital nor prehospital standard operating procedures on ApOx exist. Of the respondents 18% indicated that they regularly perform ApOx. The procedure is employed in the following scenarios: 54% for respiratory insufficiency, 42% for expected difficult airway and 34% for rapid sequence intubation. In the clinical practice 51% of procedures utilize a high-flow nasal cannula, while 33% employ a standard nasal cannula.
Conclusion: Despite the scientific evidence indicating that the utilization of ApOx is associated with a markedly reduced incidence of hypoxemia and an elevated probability of first-pass intubation success, it is not employed on a routine basis in Germany. Currently, there is an absence of standardization with respect to the indications and administration technique of ApOx. The underlying factors contributing to this phenomenon are believed to be numerous and multifaceted.
Zusammenfassung: HINTERGRUND UND FRAGESTELLUNG: Die apnoische Oxygenierung (ApOx) stellt ein Verfahren dar, welches im Rahmen der Narkoseeinleitung zur Verlängerung der sicheren Apnoezeit sowie zur Vermeidung von Desaturation zum Einsatz kommt. Trotz Erwähnung in nationalen sowie internationalen Leitlinien ist die praktische Anwendung der ApOx in Deutschland bisher nicht wissenschaftlich erfasst.
Ziel der arbeit: Die vorliegende Studie verfolgt das Ziel, die praktische Anwendung der ApOx in deutschen Kliniken aller Versorgungsstufen zu evaluieren.
Material und methoden: Zwischen 01.07.2024 und 03.09.2024 erfolgte eine multizentrische, explorative, anonyme Befragung der Anästhesisten in verschiedenen deutschen Kliniken. Die Befragung erfolgte über die Online-Plattform Lime Survey (Hamburg, Deutschland). Die Auswertung erfolgt auf Basis einer deskriptiven Statistik.
Ergebnisse: Die Umfrage wurde von insgesamt n = 310 Anästhesisten bearbeitet; nach Ausschluss der unvollständigen Datensätze konnten n = 306 Fragebogen analysiert werden. Die Mehrheit der Teilnehmer war männlich (63 %), mit einem Durchschnittsalter von 41 Jahren (± 10,4). Die Verteilung der Karrierestufen zeigte das folgende Bild: Oberarzt (34 %), Arzt in Weiterbildung (34 %), Facharzt (25 %), Chefarzt (8 %). In 84 % der Fälle konnte festgestellt werden, dass weder innerklinisch noch prähospital eine Standardarbeitsanweisung zur ApOx existierte. In der vorliegenden Studie gaben 18 % der Anästhesisten an, die ApOx regelmäßig durchzuführen. Die Anwendung erfolgt in den folgenden Situationen: 54 % „respiratorische Insuffizienz“, 42 % „erwartet schwieriger Atemweg“ und 34 % „Notfallnarkose“. Die praktische Durchführung erfolgt zu 51 % über eine High-Flow-Nasenkanüle oder zu 33 % über eine Standardnasenbrille.
Schlussfolgerung: Trotz wissenschaftlicher Evidenz, die eine signifikant geringere Hypoxämierate sowie eine erhöhte Wahrscheinlichkeit für einen „First-Pass-Intubation-Success“ bei der Anwendung der ApOx zeigt, findet diese in Deutschland aktuell keine routinemäßige Anwendung. Zum gegenwärtigen Zeitpunkt konnte keine Standardisierung hinsichtlich der Indikation und der Anwendungstechnik der ApOx festgestellt werden.
Keywords: Airway management; Anesthesia; Narcosis; Oxygen; Patient safety; Preoxygenation.
© 2025. The Author(s).
Conflict of interest statement
Einhaltung ethischer Richtlinien. Interessenkonflikt: D.D. Uzun, F. Hezel, S. Mohr, M.A. Weigand und F.C.F. Schmitt geben an, dass kein Interessenkonflikt besteht. Alle beschriebenen Untersuchungen am Menschen oder an menschlichem Gewebe wurden mit Zustimmung der zuständigen Ethikkommission, im Einklang mit nationalem Recht sowie gemäß der Deklaration von Helsinki von 1975 (in der aktuellen, überarbeiteten Fassung) durchgeführt. Von allen beteiligten Anästhesisten liegt eine Einverständniserklärung vor.
Figures
Similar articles
-
Apnoeic oxygenation in pediatric anesthesia: better safe than sorry!BMC Anesthesiol. 2025 Mar 8;25(1):116. doi: 10.1186/s12871-025-02995-2. BMC Anesthesiol. 2025. PMID: 40055595 Free PMC article.
-
Apnoeic oxygenation during paediatric tracheal intubation: a study protocol for a single-centre, cluster randomised clinical trial (ApOx-Pedi-Trial).BMJ Open. 2025 May 2;15(5):e096842. doi: 10.1136/bmjopen-2024-096842. BMJ Open. 2025. PMID: 40316345 Free PMC article.
-
Apneic nasal oxygenation and safe apnea time during pediatric intubations by learners.Paediatr Anaesth. 2019 Jun;29(6):628-634. doi: 10.1111/pan.13645. Epub 2019 Apr 29. Paediatr Anaesth. 2019. PMID: 30943324
-
A Narrative Review of Oxygenation During Pediatric Intubation and Airway Procedures.Anesth Analg. 2020 Apr;130(4):831-840. doi: 10.1213/ANE.0000000000004403. Anesth Analg. 2020. PMID: 31567323 Review.
-
The Effect of Apneic Oxygenation on Reducing Hypoxemia During Rapid Sequence Induction and Intubation in the Acutely Ill or Injured.Adv Emerg Nurs J. 2017 Oct/Dec;39(4):309-317. doi: 10.1097/TME.0000000000000168. Adv Emerg Nurs J. 2017. PMID: 29095183 Review.
References
-
- Benumof JL, Herway ST (2017) High end-tidal oxygen concentration can be a misleading sole indicator of the completeness of preoxygenation. Anesth Analg 124:2093–2093 - PubMed
-
- McNamara MJ, Hardman JG (2005) Hypoxaemia during open-airway apnoea: a computational modelling analysis. Anaesthesia 60:741–746 - PubMed
-
- Marshall SD, Pandit JJ (2016) Radical evolution: the 2015 difficult airway society guidelines for managing unanticipated difficult or failed tracheal intubation. Anaesthesia 71:131–137 - PubMed
-
- Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B (2015) S1-Leitlinie Atemwegsmanagement. Anaesthesist 64:859–873 - PubMed
-
- Piepho T, Kriege M, Byhahn C, Cavus E, Dörges V, Ilper H et al (2024) Empfehlungen zur neuen S1-Leitlinie Atemwegsmanagement. Anaesthesiologie 73:379–384 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials