

Epidemiology and prediction of non-targeted bacteria by the filmarray pneumonia plus panel in culture-positive ventilator-associated pneumonia: a retrospective multicentre analysis
- PMID: 40293547
- PMCID: PMC12037957
- DOI: 10.1186/s13613-025-01468-6
Epidemiology and prediction of non-targeted bacteria by the filmarray pneumonia plus panel in culture-positive ventilator-associated pneumonia: a retrospective multicentre analysis
Abstract
Background: Ventilator-associated pneumonia (VAP) is a prevalent nosocomial infection in intensive care units (ICUs) with significant impacts on patient outcomes and healthcare costs. Multiplex PCR could allow for personalized empirical treatment of VAP and optimize antibiotic therapy.
Methods: This multicenter retrospective study analyzed culture-positive VAP cases from January 2016 to March 2021 across 12 ICUs in France. The prevalence of non-targeted bacteria was evaluated according to the bacterial species included in the BioFire® FilmArray® Pneumonia Panel (FAPPP), and associated risk factors were identified. A non-targeted bacteria was defined as a bacterial species isolated during VAP, not included in the FilmArray panel, but considered by the clinician in the final antibiotic therapy.
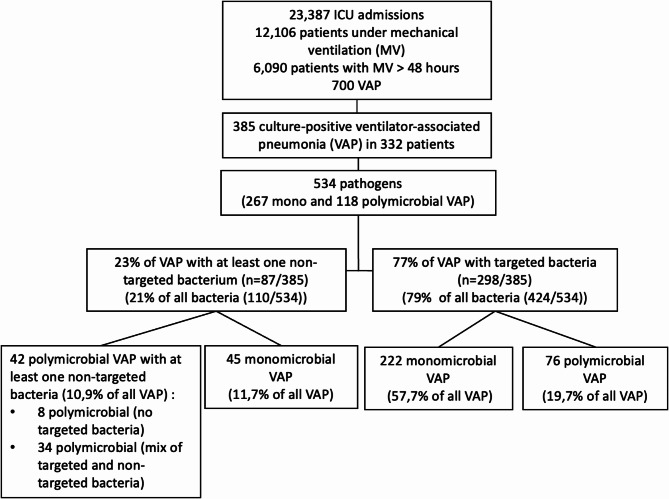
Results: Among 332 patients with 385 culture-positive VAP episodes, non-targeted pathogens were observed in 23% of cases (87/385) and represented 21% (110/534) of isolated bacteria (After excluding bacteria with low pathogenicity, the rate of VAP with a non-targeted bacterium was 21%). The most common non-targeted bacteria identified were Stenotrophomonas maltophilia (22%), Citrobacter koseri, and Hafnia alvei. Gram stain results poorly correlated with definitive cultures (42% of concordance). The proportion of culture-positive VAP with non-targeted bacteria varied significantly between ICUs, ranging from 12 to 37%, (p = 0.013). Polymicrobial culture-positive VAP had a twofold higher risk of non-targeted bacteria (47% vs. 25%, p < 0.001). In the multivariate analysis, in-ICU antibiotic exposure was associated with a twofold increased risk of non-targeted bacteria (25.3% vs. 12.9%, p = 0.042), and age over 70 years was associated with a threefold increased risk (p = 0.027). Among the 48 culture-positive VAP cases with ineffective empiric treatment, Pseudomonas aeruginosa (22%), Stenotrophomonas maltophilia (14%), and Enterobacter cloacae complex (8%) were the most frequent bacteria. Additionally, 67% of the culture-positive VAP cases with ineffective empirical antibiotic therapy involved targeted bacteria, of which 59% could have received effective empirical antibiotic therapy if panel results had been available, according to bacterial species identification and current guidelines.
Conclusions: A significant rate of culture-positive VAP cases with non-targeted bacteria was observed in this study, raising concerns about the interpretation of FAPPP results. Only positive FAPPP results may assist clinicians in the early personalization of antibiotic therapy for VAP.
Keywords: Antibiotic therapy; Bacteria; Intensive care units; Multiplex polymerase chain reaction; Rapid diagnosis; Ventilator-associated pneumonia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was authorized by the ethics committee of Angers University Hospital in March 2021 (registration number 2021-045). Consent for publication: A non-opposition letter was obtained for each included patient in accordance with current French legislation. Competing interests: All authors declare that they have no competing interests.
Figures




References
-
- Koulenti D, Tsigou E, Rello J. Nosocomial pneumonia in 27 ICUs in Europe: perspectives from the EU-VAP/CAP study. Eur J Clin Microbiol Infect Dis. 2017;36(11):1999–2006. - PubMed
-
- Melsen WG, Rovers MM, Groenwold RH, Bergmans DC, Camus C, Bauer TT, et al. Attributable mortality of ventilator-associated pneumonia: a meta-analysis of individual patient data from randomised prevention studies. Lancet Infect Dis. 2013;13(8):665–71. - PubMed
-
- Bekaert M, Timsit JF, Vansteelandt S, Depuydt P, Vésin A, Garrouste-Orgeas M, et al. Attributable mortality of Ventilator-Associated pneumonia: A reappraisal using causal analysis. Am J Respir Crit Care Med. 2011;184(10):1133–9. - PubMed
-
- Zhu S, Wang W, Kang Y, He Q, Zhang H, Deng Y, et al. Clinical outcomes and risk factors for mortality from ventilator-associated events: A registry-based cohort study among 30,830 intensive care unit patients. Infect Control Hosp Epidemiol. 2022;43(1):48–55. - PubMed
-
- Branch-Elliman W, Wright SB, Howell MD. Determining the ideal strategy for Ventilator-associated pneumonia prevention. Cost–Benefit analysis. Am J Respir Crit Care Med. 2015;192(1):57–63. - PubMed
LinkOut - more resources
Full Text Sources
