

Follow-up of bowel endometriosis resections performed using the double circular stapler technique: A decade's experience
- PMID: 40294015
- PMCID: PMC12036926
- DOI: 10.1371/journal.pone.0320138
Follow-up of bowel endometriosis resections performed using the double circular stapler technique: A decade's experience
Abstract
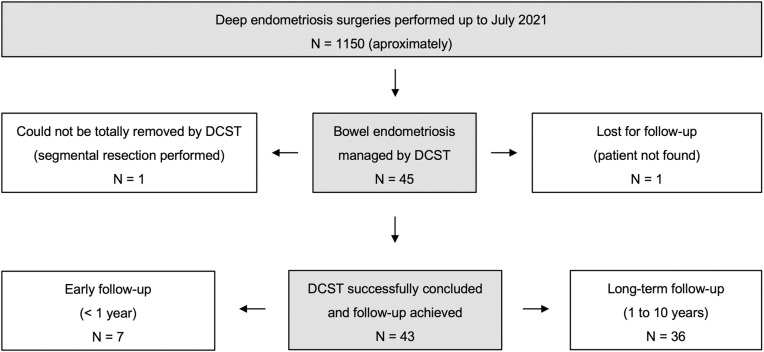
Study objective: To report individual early and long-term functional outcomes of 43 women who underwent double circular stapler technique (DCST) for colorectal deep endometriosis (DE).
Methods: This multidisciplinary observational study was a retrospective case series report exploiting a long-established database of clinical information from a single private institution. The cohort consists of consecutive patients from January/2010 through July/2021 who underwent minimally invasive surgical treatment of DE. Inclusion criteria: all women whose bowel DE was managed by DCST. The assessment of bowel function was based on Obstructed Defecation Syndrome score, Gastrointestinal Symptom Rating Scale and Bowel Function in the Community Tool. Outcomes also included intra and postoperative complications, lower urinary tract symptoms, endometriosis-related menstrual and nonmenstrual pain (numeric rating scale), and conception. The analysis of the results was guided by a semi-qualitative reasoning based on individual changes.
Results: The follow-up ranged from 1.4 to 123.8 months (median 38.2). All women presented with DE (mostly rASRM stage 4) and underwent large resections. No procedure was converted to open surgery nor required blood transfusion or ostomies. There was no anastomotic leakage. The risk of rectovaginal bowel fistula was 2.3% (CI 95%: <0.1-7.0) - one case. No patient had long-term urinary retention after surgery. At the most recent follow-up on dysuria, dyschezia, dysmenorrhea, dyspareunia and cyclic low back pain, 88 to 100% of women had favorable responses (improvements ≥ 3 points in symptomatic women or asymptomatic women who remained pain-free). One patient reported important worsening of her intestinal function, requiring continuous use of laxatives. Considering the 20 women with pregnancy intent, 14 (70%) conceived after surgery.
Discussion / conclusion: Preliminary results were encouraging in the past. The current assessment including long-term follow-up supports DCST for colorectal DE as a feasible, useful, and safe strategy for avoiding segmental colorectal resection when appropriately indicated and properly performed.
Copyright: © 2025 Crispi Jr et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Laparoscopic Double Discoid Resection With a Circular Stapler for Bowel Endometriosis.J Minim Invasive Gynecol. 2015 Sep-Oct;22(6):929-31. doi: 10.1016/j.jmig.2015.04.021. Epub 2015 Apr 29. J Minim Invasive Gynecol. 2015. PMID: 25937595
-
Lesion size and location in deep infiltrating bowel endometriosis: Correlation with gastrointestinal dysfunction and pain.Acta Obstet Gynecol Scand. 2024 Sep;103(9):1764-1770. doi: 10.1111/aogs.14921. Epub 2024 Jul 22. Acta Obstet Gynecol Scand. 2024. PMID: 39039771 Free PMC article.
-
Ghost Ileostomy in Anterior Resection for Bowel Endometriosis: Technical Description.J Minim Invasive Gynecol. 2020 Jul-Aug;27(5):1014-1016. doi: 10.1016/j.jmig.2019.09.769. Epub 2019 Sep 12. J Minim Invasive Gynecol. 2020. PMID: 31521860
-
Surgical Outcomes after Colorectal Surgery for Endometriosis: A Systematic Review and Meta-analysis.J Minim Invasive Gynecol. 2021 Mar;28(3):453-466. doi: 10.1016/j.jmig.2020.08.015. Epub 2020 Aug 22. J Minim Invasive Gynecol. 2021. PMID: 32841755
-
Choosing the right surgical technique for deep endometriosis: shaving, disc excision, or bowel resection?Fertil Steril. 2017 Dec;108(6):931-942. doi: 10.1016/j.fertnstert.2017.09.006. Fertil Steril. 2017. PMID: 29202966 Review.
References
-
- Zondervan K, Becker C, Missmer S. Endometriosis. N Engl J Med. 2020;382(12):1244–56. - PubMed
-
- de Freitas Fonseca M, Aragao LC, Sessa FV, Dutra de Resende JA Jr, Crispi CP. Interrelationships among endometriosis-related pain symptoms and their effects on health-related quality of life: a sectional observational study. Obstet Gynecol Sci. 2018;61(5):605–14. doi: 10.5468/ogs.2018.61.5.605 - DOI - PMC - PubMed
-
- de Resende Júnior JAD, Crispi CP, Cardeman L, Buere RT, Fonseca MF. Urodynamic observations and lower urinary tract symptoms associated with endometriosis: a prospective cross-sectional observational study assessing women with deep infiltrating disease. Int Urogynecol J. 2018;29(9):1349–58. - PubMed
-
- Cornillie F, Oosterlynck D, Lauweryns JM, Koninckx PR. Deeply infiltrating pelvic endometriosis: histology and clinical significance. Fertil Steril. 1990;53(6):978–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
