

Effect of Thrombolytics on Delayed Reperfusion After Incomplete Thrombectomy: Target Trial Emulation
- PMID: 40294370
- PMCID: PMC12042098
- DOI: 10.1212/WNL.0000000000213641
Effect of Thrombolytics on Delayed Reperfusion After Incomplete Thrombectomy: Target Trial Emulation
Abstract
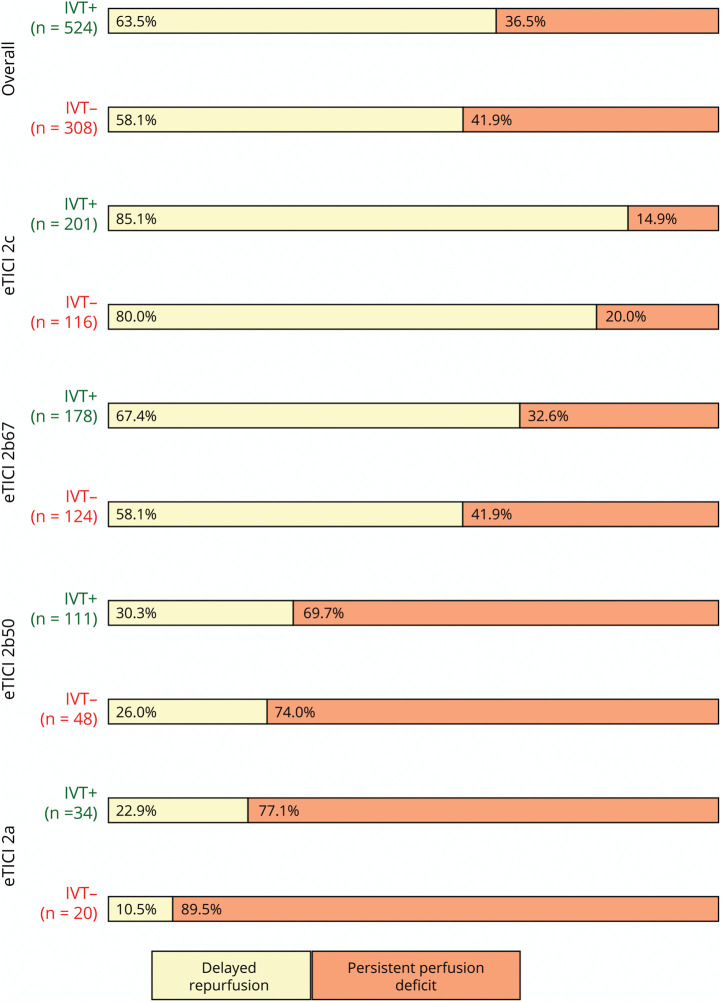
Background and objectives: More than half of the endovascularly treated ischemic stroke patients with incomplete reperfusion (expanded Thrombolysis in Cerebral Infarction [eTICI] <3) show delayed reperfusion (DR) on 24-hour perfusion imaging, which is associated with favorable clinical outcome. The effect of intravenous thrombolysis (IVT) on the rates of DR remains unclear. This study aimed to assess the treatment effect of IVT on the occurrence of DR.
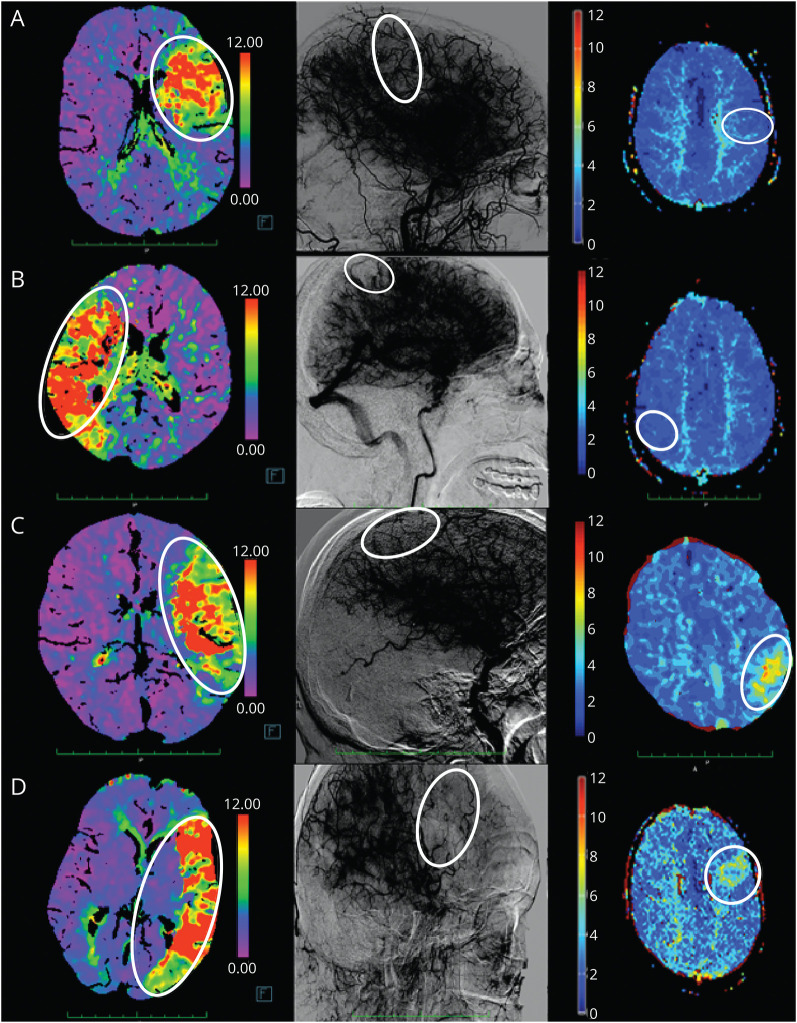
Methods: Pooled data from 3 randomized controlled trials (EXTEND-IA and EXTEND-IA TNK parts 1 and 2) and 2 comprehensive stroke centers (University Hospitals Graz and Bern) were analyzed. Only patients with a final reperfusion score of eTICI 2a-2c and available perfusion imaging at follow-up of 24 ± 12 hours were included. The primary outcome was the presence of DR on 24-hour follow-up CT/MRI perfusion imaging, defined as the absence of any focal perfusion deficit on perfusion imaging, despite incomplete reperfusion on the final angiography series during thrombectomy. For the secondary analysis, we explored the association between the primary outcome (DR) and the time elapsed between start of IVT and the end of an intervention. To address confounding in observational data, we performed a target trial emulation.
Results: Of 832 included patients with eTICI 2a-2c (median age 74 years, 49% female), 511 (61%) had DR. There was an independent treatment effect of IVT on DR (standardized risk ratio [sRR] 1.1, 95% CI 1.0-1.3; standardized risk difference [sRD] 8.2%, 95% CI 0.2%-16.1%), after adjusting for age, sex, atrial fibrillation, number of device passes, collateral score, and eTICI. Among those patients who have received IVT (n = 524/832, 63%), when adjusting for the aforementioned covariates, there was a causal effect of shorter time between administration of thrombolytics and end of the intervention on DR (sRR 0.93%, 95% CI 0.87-0.98; sRD -5.2%; 95% CI -9.1% to -1.3%, per hour increase).
Discussion: Exposure to thrombolytics showed independent treatment effect on the occurrence of DR among patients with incomplete reperfusion after thrombectomy who undergo perfusion imaging at the 24-hour follow-up. The effect of thrombolytics on DR was observed if there was a high chance of therapeutic concentrations of thrombolytics at the time point when the proximal vessel was recanalized, but distal occlusions persisted and/or occurred.
Classification of evidence: This study is rated Class III because it is a nonrandomized study and there are substantial differences in baseline characteristics of the treatment groups.
Conflict of interest statement
A. Mujanovic reports financial support from the Swiss National Science Foundation (fees paid to institution). V. Yogendrakumar reports no disclosures relevant to the manuscript. F.C. Ng reports support by the Australian National Health Medical Research Council and National Heart Foundation in research fellowships. T. Gattringer reports research grant from the Austrian Science Foundation and also reports the following: BMS Pfizer: speakers' honoraria, travel support; Bayer: speakers' honoraria, travel support; Boehringer Ingelheim: speakers' honoraria, travel support, advisory board; Novartis: speakers' honoraria, advisory board; Astra Zeneca: speakers' honoraria, advisory board. B.L. Serrrallach, T.R. Meinel, L. Churilov, O. Nistl, S. Zheng, P.J. Mitchell, N. Yassi, M.W. Parsons, G.J. Sharma, H.A. Deutschmann, G.A. Donnan, M. Arnold, F. Cavalcante, E.I. Piechowiak, T.J. Kleining, D.J. Seiffge, and S.M. Davis report no disclosures relevant to the manuscript. T. Dobrocky reports Microvention consultancy. J. Gralla and M. Kneihsl report no disclosures relevant to the manuscript. U. Fischer is a PI of ELAN, is co-PI of DISTAL, TECNO, SWIFT DIRECT trials; has research grants from Medtronic, Stryker, Rapid Medical, Penumbra, and Phenox; has consultancies for Medtronic, Stryker, and CSL Behring; is part of advisory boards for Alexion/Portola, Boehringer Ingelheim, Biogen, and Acthera; is part of clinical event committees for the COATING trial and the DSMBs of the TITAN, LATE_MT, and IN EXTREMIS trials; and is president of the Swiss Neurologic Society. All fees are paid to the institutions. B.C.V. Campbell reports no disclosures relevant to the manuscript. J. Kaesmacher reports Microvention consultancy within the framework of a corelab; financial support from Medtronic for the BEYOND SWIFT registry and SWIFT DIRECT trial; medication supply support from Boheringer-Ingelheim for the TECNO trial; a research agreement with Siemens Healthineers regarding flat panel perfusion imaging; and research grants from the Swiss National Science Foundation supporting the TECNO trial, Swiss Academy of Medical Sciences supporting MRI research, and Swiss Heart Foundation supporting cardiac MRI in the aetiological work-up of stroke patients. All fees are paid to the institutions. Go to
Figures

References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. . Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart association/American stroke association. Stroke. 2019;50(12):e344-e418. doi:10.1161/STR.0000000000000211 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials