

Minimally invasive radical prostatectomy versus open radical prostatectomy: A systematic review and meta-analysis of randomized control trials
- PMID: 40294454
- PMCID: PMC12059318
- DOI: 10.1016/j.clinsp.2025.100636
Minimally invasive radical prostatectomy versus open radical prostatectomy: A systematic review and meta-analysis of randomized control trials
Abstract
Objective: To evaluate the comparative outcomes of Minimally Invasive Radical Prostatectomy (MIRP) versus Open Radical Prostatectomy (ORP) to treat localized prostate cancer, using only Randomized Controlled Trials (RCTs) to ensure high-quality evidence.
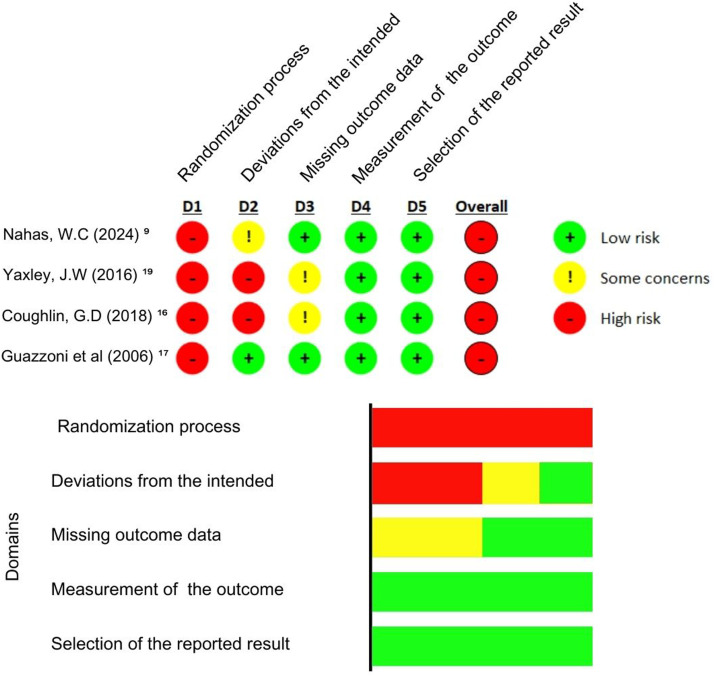
Method: A systematic review and meta-analysis were conducted in accordance with PRISMA guidelines, focusing solely on RCTs comparing MIRP (robot-assisted or laparoscopic surgery) and ORP. Literature searches across multiple databases, including Cochrane Library, Medline, Embase, Lilacs, Scopus, Web of Science, NIH, Clinical Trials, and EU Clinical Trials Register, identified studies meeting predefined PICOT criteria. Four RCTs met inclusion criteria ‒ two representing the same cohort of patients ‒ and were analyzed for perioperative, functional, and oncologic outcomes. Quality assessment utilized the ROB-2 tool to gauge the risk of bias.
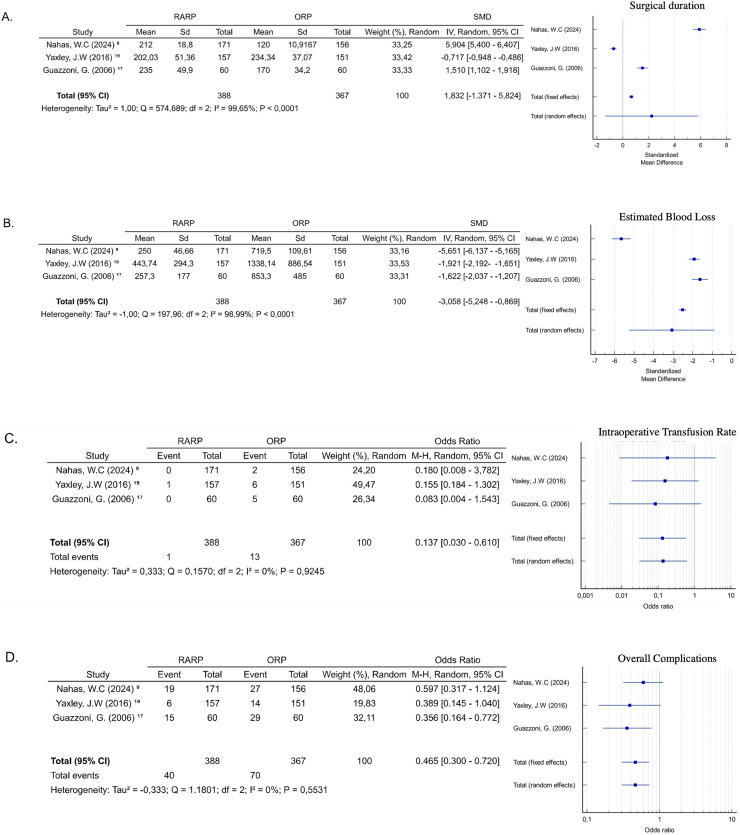
Results: Three RCTs encompassing 1051 patients were analyzed. MIRP demonstrated statistically significant benefits over ORP in terms of reduced perioperative blood loss (Standardized Mean Difference [SMD = -3.058], p = 0.006), lower transfusion rates (Odds Ratio [OR = 0.137]; p = 0.009), and fewer overall complications (OR = 0.465; p = 0001). However, no significant differences were found in long-term oncologic and functional outcomes, including urinary continence and erectile function. Positive surgical margins and additional treatments also did not differ significantly between groups.
Conclusion: This systematic review and meta-analysis of RCTs indicated that MIRP offers perioperative advantages over ORP, supporting its role as a safe and effective option for localized prostate cancer.
Keywords: Meta-Analysis; Open radical prostatectomy; Prostate cancer; Randomized Control Trial; Robot-assisted radical prostatectomy.
Copyright © 2025 HCFMUSP. Published by Elsevier España, S.L.U. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare no conflicts of interest.
Figures



References
-
- Sung H., Ferlay J., Siegel R.L., Laversanne M., Soerjomataram I., Jemal A., et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. - PubMed
-
- Siegel R.L., Miller K.D., Fuchs H.E., Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. - PubMed
-
- Evans S.M., Millar J.L., Davis I.D., Murphy D.G., Bolton D.M., Giles G.G., et al. Patterns of care for men diagnosed with prostate cancer in Victoria from 2008 to 2011. Med J Aust. 2013;198(10):540–545. - PubMed
-
- Hamdy F.C., Donovan J.L., Lane J.A., Mason M., Metcalfe C., Holding P., et al. ProtecT Study group. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375(15):1415–1424. - PubMed
-
- Binder J., Kramer W. Robotically-assisted laparoscopic radical prostatectomy. BJU Int. 2001;87(4):408–410. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
