

Current status and prospects of endovascular treatment for intracranial vertebral artery aneurysms: A narrative review
- PMID: 40295275
- PMCID: PMC12040039
- DOI: 10.1097/MD.0000000000042265
Current status and prospects of endovascular treatment for intracranial vertebral artery aneurysms: A narrative review
Abstract
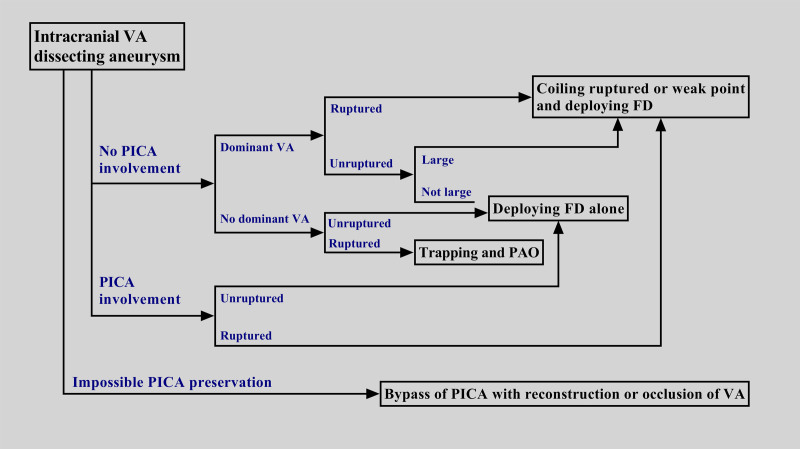
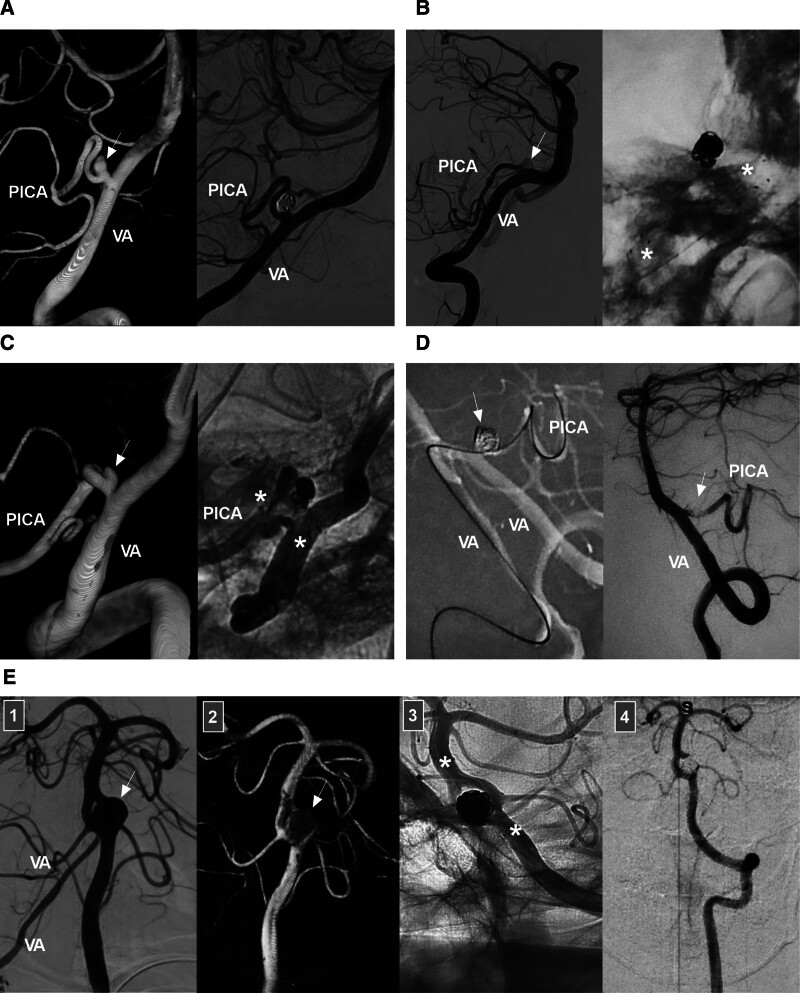
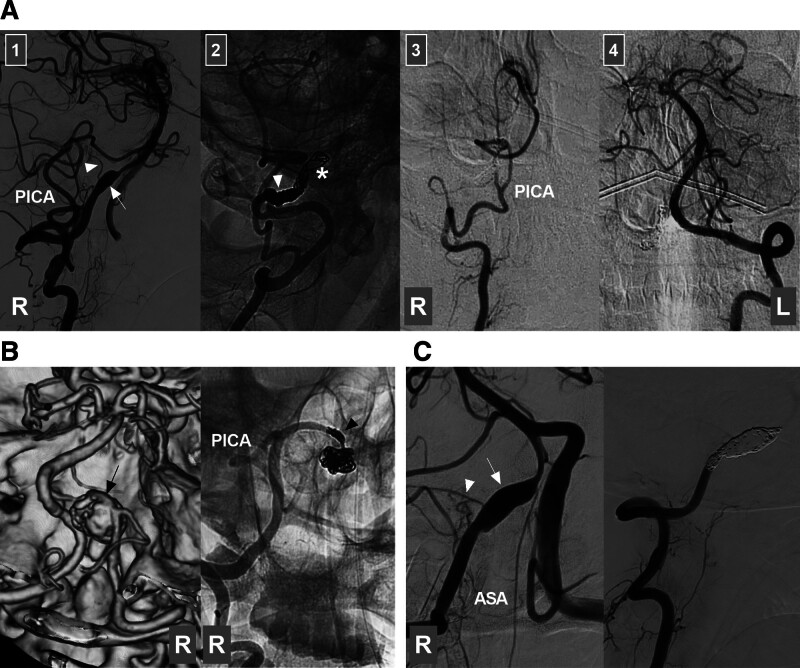
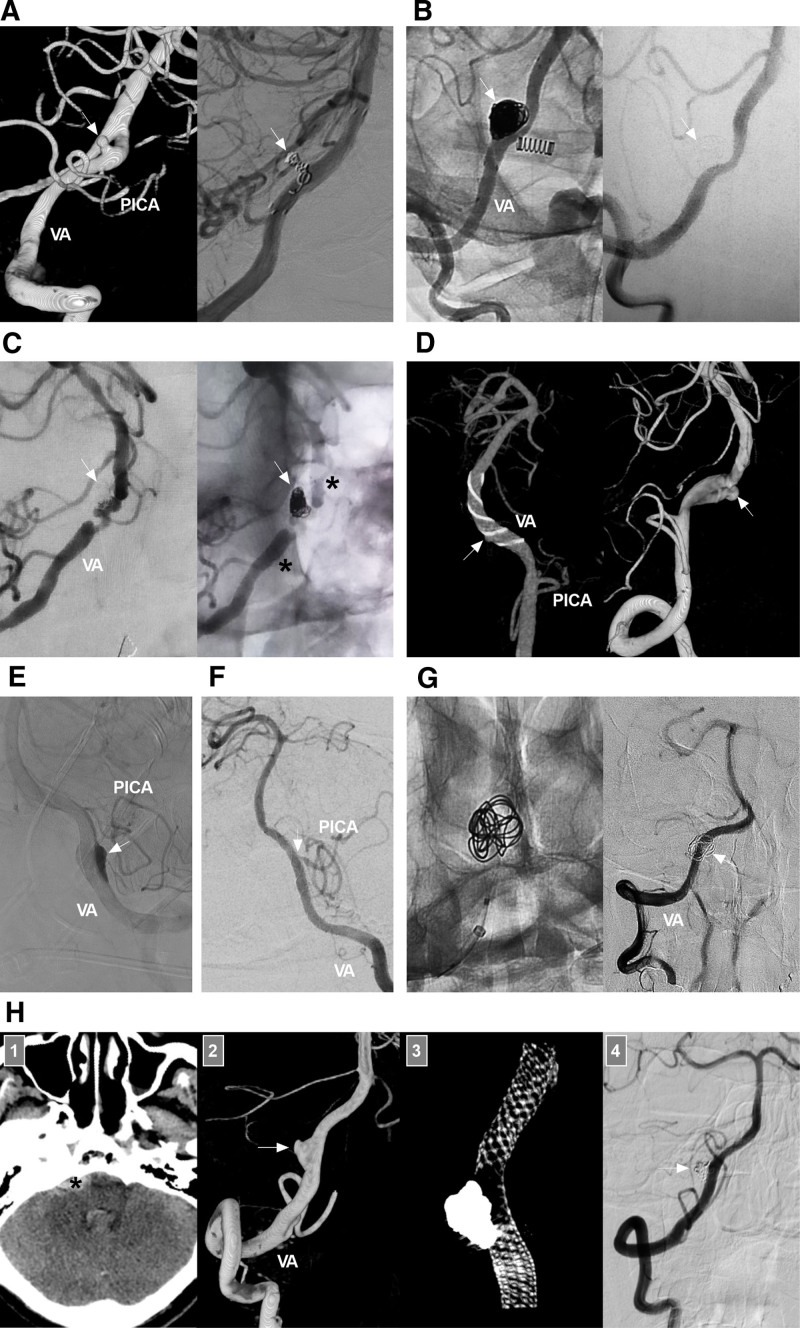
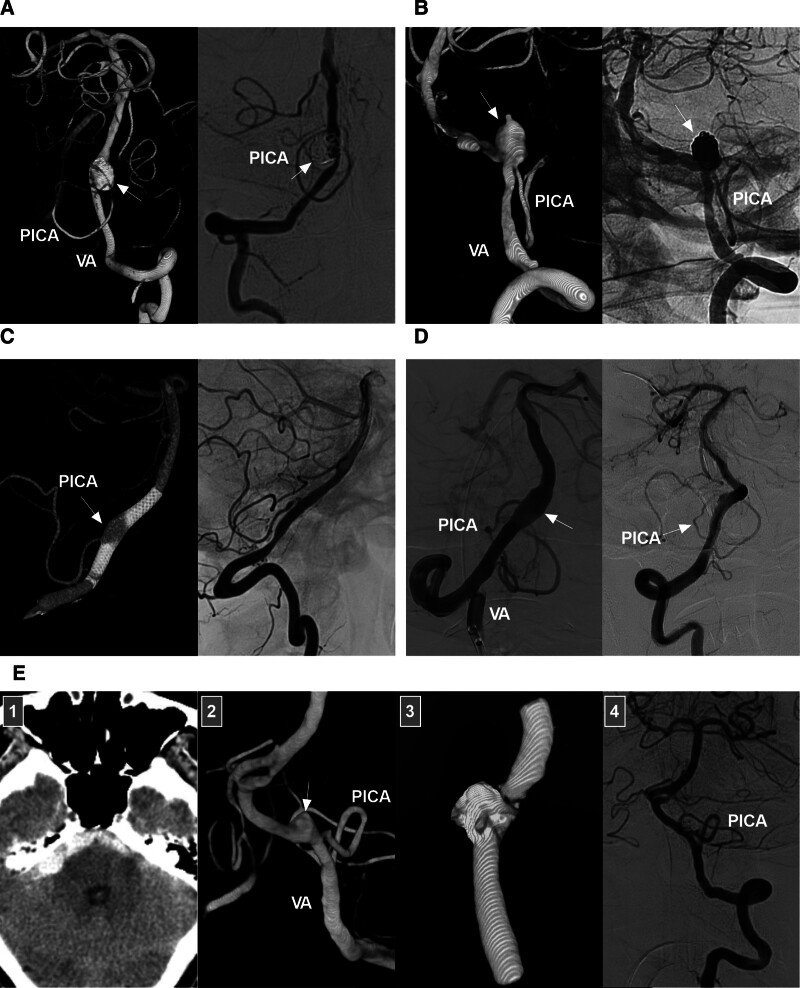
Intracranial vertebral artery (VA) aneurysms are complex entities. Endovascular treatment (EVT) can be used to treat intracranial VA aneurysms. Nevertheless, managing these lesions with EVT remains challenging. Moreover, the suitability of EVT for every type of intracranial VA aneurysm has not been fully confirmed. Therefore, we conducted a needed review of the current literature and our experience summarizing the current status of and advancements in EVT in the management of intracranial VA aneurysms. In our review, several issues are discussed, including the anatomy and anomalies of the intracranial VA, the classification and natural history of intracranial VA aneurysms, indications and techniques for EVT in the management of intracranial VA aneurysms, and the outcomes of and complications experienced by patients who undergo EVT. A flowchart describing EVT options for dissecting intracranial VA aneurysms derived from the findings of this review and our experience is provided. The key to successful EVT is preservation of the posterior inferior cerebellar artery and avoidance of injury to any brainstem perforators. Currently, intracranial VA reconstruction via flow diverter deployment plays an important role in achieving successful treatment. For appropriate cases, both reconstructive and deconstructive EVT can result in good patient outcomes. However, EVT-related complications should be considered. If management of complex intracranial VA aneurysms with EVT would be expected to disproportionally harm the patient, extracranial-intracranial bypass and aneurysmectomy are often necessary. In addition, new products and techniques that show promise for achieving successful EVT in the management of intracranial VA aneurysms are described.
Keywords: aneurysm; endovascular treatment; intracranial vertebral artery; prognosis; review.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Vertebral artery-posterior inferior cerebellar artery bypass using a radial artery graft for hemorrhagic dissecting vertebral artery aneurysms: surgical technique and report of 2 cases.J Neurosurg. 2011 Apr;114(4):1074-9. doi: 10.3171/2010.5.JNS091435. Epub 2010 Jun 11. J Neurosurg. 2011. PMID: 20540594
-
Endovascular treatment of posterior inferior cerebellar artery trunk aneurysm.Acta Neurol Belg. 2022 Dec;122(6):1405-1417. doi: 10.1007/s13760-021-01826-8. Epub 2021 Oct 22. Acta Neurol Belg. 2022. PMID: 34677822 Review.
-
Combined microsurgical PICA-PICA bypass and endovascular parent artery occlusion for a ruptured dissecting vertebral artery aneurysm.Neurosurg Focus. 2015 Jan;38(VideoSuppl1):Video3. doi: 10.3171/2015.V1.FOCUS14526. Neurosurg Focus. 2015. PMID: 25554844
-
Intracranial-to-intracranial bypass for posterior inferior cerebellar artery aneurysms: options, technical challenges, and results in 35 patients.J Neurosurg. 2016 May;124(5):1275-86. doi: 10.3171/2015.5.JNS15368. Epub 2015 Nov 13. J Neurosurg. 2016. PMID: 26566199
-
Endovascular treatment for aneurysms at the A1 segment of the anterior cerebral artery: current difficulties and solutions.Acta Neurol Belg. 2021 Feb;121(1):55-69. doi: 10.1007/s13760-020-01526-9. Epub 2020 Oct 27. Acta Neurol Belg. 2021. PMID: 33108602 Review.
References
-
- Lehto H, Niemelä M, Kivisaari R, et al. . Intracranial vertebral artery aneurysms: clinical features and outcome of 190 patients. World Neurosurg. 2015;84:380–9. - PubMed
-
- Durongwatana N, Sriamornrattanakul K, Wongsuriyanan S, Akharathammachote N. Microsurgical treatment of vertebral artery dissection: surgical strategies and treatment outcomes. World Neurosurg. 2022;159:e375–88. - PubMed
-
- Lv X, Lv M, Li Y, Yang X, Jiang C, Wu Z. Endovascular treatment of ruptured and unruptured vertebral artery aneurysms. Neuroradiol J. 2011;24:677–86. - PubMed
-
- Hernández-Durán S, Ogilvy CS. Clinical outcomes of patients with vertebral artery dissection treated endovascularly: a meta-analysis. Neurosurg Rev. 2014;37:569–77. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
