

A New Predictive Parameter for Rotator Cuff Tears: Acromial Incidence Angle
- PMID: 40297048
- PMCID: PMC12035219
- DOI: 10.1177/23259671251331057
A New Predictive Parameter for Rotator Cuff Tears: Acromial Incidence Angle
Abstract
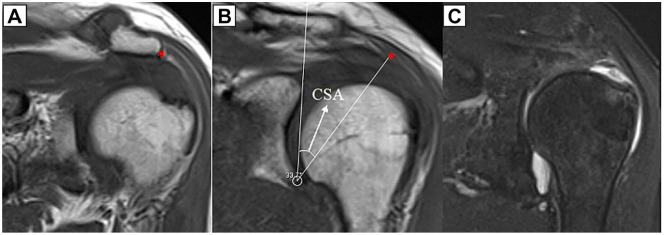
Background: A significant statistical association of increased critical shoulder angle (CSA) with rotator cuff tear (RCT) has been demonstrated; however, the mean difference between RCT and control groups varies between approximately 1° and 3.5°, with a wide range of distribution of the CSA from 18° to 55°. It may be more predictive to evaluate the CSA in conjunction with parameters that evaluate the morphology of the acromion in the sagittal plane.
Hypothesis: It was hypothesized that the acromial incidence angle (AIA), which can evaluate the position and orientation of the acromion in the sagittal plane, may be associated with RCT and that AIA, when evaluated together with the CSA, may provide a highly predictive measure of risk for RCT.
Study design: Cross-sectional study; Level of evidence, 3.
Methods: The study included 117 patients who underwent arthroscopic repair for posterosuperior RCT and 117 patients as a control group. The CSA, AIA, glenoid inclination, glenoid version, and anterior acromial coverage were measured on magnetic resonance imaging. The groups were compared in terms of these parameters.
Results: The mean CSA was significantly higher in the RCT group (35.7°± 5.3°) than in the control group (33.9°± 4.5°), with a sensitivity of 57.1% and a specificity of 61.3% (P = .009). The mean AIA was also significantly higher in the RCT group (77.4°± 12.9°) compared with the control group (63.7°± 9.4°), with a sensitivity of 80.2% and a specificity of 83.9% (P < .001). The anterior acromial coverage showed significantly less anterior coverage in the RCT group (-16.5°± 14°) than in the control group (-9.7°± 10.5°) (P = .033). Logistic regression analysis showed that the CSA and the AIA were associated with RCT independently of other parameters (P < .001, P < 0.001, odds ratio [OR], 1.32, and OR, 1.34, respectively). In the patient group with a CSA of <35°, AIA values of >72° predicted RCT with a sensitivity of 85.6% and a specificity of 84.8%, while in the patient group with a CSA of ≥35°, values of >65° predicted RCT, with a sensitivity of 70.2% and a specificity of 76.7%.
Conclusion: The AIA predicted RCT with a sensitivity of 80.2% and a specificity of 83.9% for values >70°. In patients with a CSA of <35°, it predicted RCT, with a sensitivity of 85.6% and a specificity of 84.8% at values >72°. By evaluating the relationship between the acromion and the glenoid in the sagittal plane, the AIA, as a novel parameter, allows for the reevaluation of the risk in the patient group with a CSA of <35°, which is considered to be in the low-risk category in terms of RCT.
Keywords: acromial incidence angle; acromial morphology; anterior acromial coverage; critical shoulder angle; rotator cuff tear.
© The Author(s) 2025.
Conflict of interest statement
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from Necmettin Erbakan University Ethical Committee (Reference No. 2024-5056).
Figures





References
-
- Arner JW, Nolte P-C, Ruzbarsky JJ, et al.. Correlation of acromial morphology with risk and direction of shoulder instability: an MRI study. Am J Sports Med. 2023;51(12):3211-3216. - PubMed
-
- Beeler S, Hasler A, Getzmann J, Weigelt L, Meyer DC, Gerber C. Acromial roof in patients with concentric osteoarthritis and massive rotator cuff tears: multiplanar analysis of 115 computed tomography scans. J Shoulder Elbow Surg. 2018;27(10):1866-1876. - PubMed
-
- Bigliani L. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans. 1986;10:228.
-
- Bjarnison AO, Sørensen TJ, Kallemose T, Barfod KW. The critical shoulder angle is associated with osteoarthritis in the shoulder but not rotator cuff tears: a retrospective case-control study. J Shoulder Elbow Surg. 2017;26(12):2097-2102. - PubMed
-
- Blonna D, Giani A, Bellato E, et al.. Predominance of the critical shoulder angle in the pathogenesis of degenerative diseases of the shoulder. J Shoulder Elbow Surg. 2016;25(8):1328-1336. - PubMed
LinkOut - more resources
Full Text Sources
