

Association between admission Braden Skin Score and delirium in surgical intensive care patients: an analysis of the MIMIC-IV database
- PMID: 40297853
- PMCID: PMC12036481
- DOI: 10.3389/fneur.2025.1555166
Association between admission Braden Skin Score and delirium in surgical intensive care patients: an analysis of the MIMIC-IV database
Abstract
Background: The Braden Skin Score (BSS), a tool for assessing pressure ulcers, is increasingly recognized for its prognostic value in various disorders. However, its link to critical delirium in surgical patients remains understudied. This study aimed to explore the association between BSS upon admission and the risk of delirium in SICU patients.
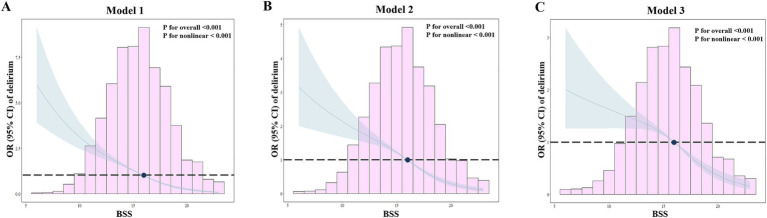
Methods: This retrospective observational cohort study used data from the Medical Information Mart for Intensive Care (MIMIC)-IV database. The primary outcome was incidence of delirium. Feature importance of BSS was initially assessed using a machine learning algorithm, while restricted cubic spline (RCS) models and multivariable logistic analysis evaluated the relationship between BSS and delirium. Additionally, Kaplan-Meier analysis and mediation analysis were conducted to explore interactions among BSS, delirium, and short-term mortality.
Results: A total of 4,899 patients were included in the study, among whom 1,491 were diagnosed with delirium. The Boruta algorithm identified BSS as a significant predictor of delirium occurrence. RCS models demonstrated a non-linear positive relationship between BSS and delirium. Based on RCS curves, the optimal threshold for BSS was established at 16, thereby categorizing participants into two groups: those with BSS < 16 and those with BSS ≥ 16. Multivariable logistic regression analysis revealed that lower BSS was positively correlated with an increased risk of delirium. These findings exhibited robust consistency across subgroup analyses and sensitivity analyses. Furthermore, patients in lower BSS groups had a higher 90-day mortality, with delirium mediating an indirect effect on this outcome.
Conclusion: The low BSS was independently associated with an increased risk of delirium in critically ill surgical patients. Patients exhibiting a BSS below 16 demonstrated heightened susceptibility to the onset of delirium, thereby necessitating vigilant monitoring and timely intervention. Larger prospective studies are needed to confirm these findings.
Keywords: Braden Skin Score; MIMIC-IV database; delirium; risk factors; surgical intensive care unit.
Copyright © 2025 Shang, Shang and Xu.
Conflict of interest statement
The authors declare that the research was conducted without any commercial or financial relationships that could be seen as a conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources