

Elevated Triglyceride-Glucose Index Is Associated With Insulin Resistance, Metabolic Syndrome Components, Nonalcoholic Fatty Liver Disease, and Adverse Pregnancy Outcomes in Chinese Women With Polycystic Ovary Syndrome
- PMID: 40298068
- PMCID: PMC12319269
- DOI: 10.1111/cen.15252
Elevated Triglyceride-Glucose Index Is Associated With Insulin Resistance, Metabolic Syndrome Components, Nonalcoholic Fatty Liver Disease, and Adverse Pregnancy Outcomes in Chinese Women With Polycystic Ovary Syndrome
Abstract
Aim: To investigate the associations of triglyceride-glucose index (TyG) with anthropometric characteristics, metabolic/endocrine profiles, and pregnancy outcomes in Chinese women with polycystic ovary syndrome (PCOS).
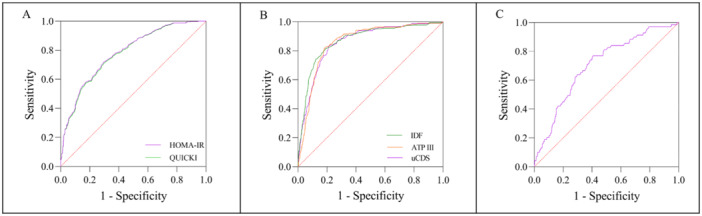
Methods: This secondary analysis of the Acupuncture and Clomiphene for Chinese Women with Polycystic Ovary Syndrome trial (PCOSAct) included 956 participants with prospectively collected data. TyG was calculated using fasting triglyceride and glucose levels (Ln [TG (mg/dL) × FPG (mg/dL)/2]). Linear regression and trend analyses evaluated relationships between TyG and clinical parameters. Receiver operating characteristic (ROC) curves assessed TyG's predictive capacity for insulin resistance (IR), metabolic syndrome (MS), and nonalcoholic fatty liver disease (NAFLD). Multivariable logistic regression estimated risks for metabolic outcomes and pregnancy outcomes.
Results: Linear trends revealed that the TyG was positively associated with age, body mass index (BMI), waist circumference, hip circumference, waist-to-hip ratio, systolic blood pressure, diastolic blood pressure, FPG, fasting insulin, the homeostatic model assessment for insulin resistance (HOMA-IR), total cholesterol, triglycerides, low-density lipoprotein (LDL), apolipoprotein B, free androgen index, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and the prevalence of IR, MS, and NAFLD across various standards. Conversely, TyG was negatively correlated with the quantitative insulin sensitivity check index (QUICKI), high-density lipoprotein (HDL), apolipoprotein A1, sex hormone-binding globulin (SHBG), and the prevalence of ovulation per cycle, conception, pregnancy, and live birth. After adjusting for age and BMI, a significant linear relationship was observed between TyG and components of MS, IR markers, and ALT. The ROC curve analysis indicated that the AUCMS-IDF was 0.871 (95% CI: 0.846-0.896), with a sensitivity of 81.4% and specificity of 81.2% at a cut-off value of 8.745, and the AUCIR-HOMA-IR was 0.782 (95% CI: 0.753-0.811), with 71.9% sensitivity and 70.3% specificity at a cut-off of 8.585, and the AUCNAFLD was 0.705 (95% CI: 0.644-0.766), with 76.8% sensitivity and 59.3% specificity at a cut-off value of 8.665. Logistic regression analysis demonstrated that participants in the highest quartile (Q4) of TyG had significantly higher odds ratios (OR) for MS (OR: 38.36, 95% CI: 20.03-73.46, P-trend < 0.001) and IR (OR: 12.49, 95% CI: 7.3-21.35, P-trend < 0.001) compared to those in the lowest quartile (Q1), while NAFLD showed a marginal association (OR: 2.56, 95% CI: 1.00-6.55, P-trend = 0.069) after adjusting for confounding factors. Conversely, participants in Q1 of TyG had higher OR of conception (OR: 1.56, 95% CI: 1.04-2.35, p < 0.05), pregnancy (OR: 2.35, 95% CI: 1.46-3.79, p < 0.01), and live birth (OR: 2.32, 95% CI: 1.42-3.78, p < 0.01) compared to those in Q4 after adjusting for treatments.
Conclusions: Elevated TyG index strongly associates with adverse metabolic trajectories, and adverse pregnancy outcomes in PCOS patients. This biomarker shows particular utility for identifying metabolic dysfunction, suggesting clinical potential for risk stratification in PCOS management.
Keywords: insulin resistance; metabolic syndrome; nonalcoholic fatty liver disease; polycystic ovary syndrome; pregnancy outcomes; triglyceride‐glucose index.
© 2025 The Author(s). Clinical Endocrinology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
