

Feasibility of the CT-Image-Guided Colpopexy: A Novel, Needle-Based Sacrospinous Ligament Fixation for Treatment of Vaginal Apical Prolapse
- PMID: 40298957
- PMCID: PMC12182468
- DOI: 10.1007/s00192-025-06083-4
Feasibility of the CT-Image-Guided Colpopexy: A Novel, Needle-Based Sacrospinous Ligament Fixation for Treatment of Vaginal Apical Prolapse
Abstract
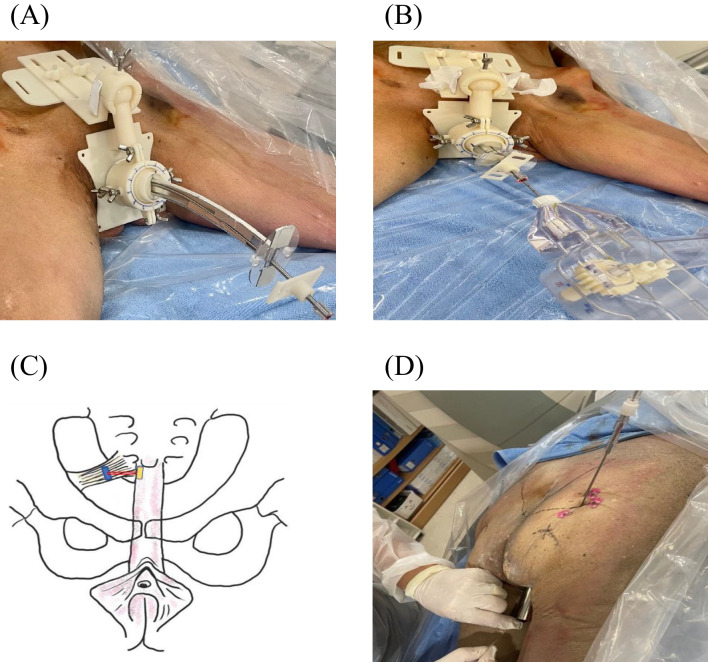
Introduction and hypothesis: Although several procedures have been developed to increase the precision and reduce the invasiveness of sacrospinous ligament fixation surgery, all surgical approaches require dissection of the vagina to access the paravaginal space and visual or tactile identification of the ligament before deploying a suture or anchor device at the ligament target site. The aim of this study was to develop and demonstrate the feasibility of a minimally invasive, needle-based treatment of vaginal apical prolapse by CT-image-guided anchoring of the vaginal vault to the sacrospinous ligament in cadavers.
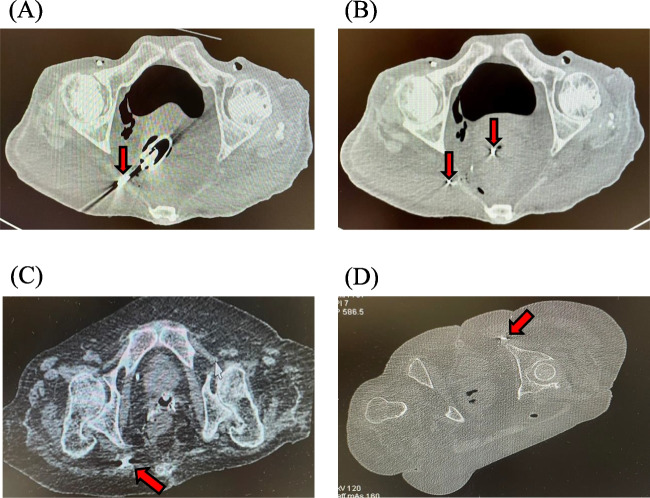
Methods: A CT-image-guided, needle-based colpopexy procedure was performed on six female cadavers. After the placement of the vaginal probe, each cadaver was CT scanned to identify the target sacrospinous ligament. An anchoring device was inserted through the vaginal probe toward the target ligament. Small anchors, introduced through needle lumens via either transvaginal or transgluteal access, were implanted under the guidance of CT images to anchor the vaginal vault to the sacrospinous ligament. The cadavers were dissected and compared with CT images to evaluate the anatomical locations of the anchors with respect to the anatomical landmarks in the pelvis. Pull-out forces of the implants were also measured.
Results: Thirty-two anchors were inserted via transvaginal access, whereas ten anchors were inserted via transgluteal access. CT images revealed that the inserted anchors were implanted in the sacrospinous ligaments (n = 40: 30 transvaginal and 10 transgluteal) or sacrotuberous ligaments (n = 2: transvaginal), as confirmed by dissection of the gluteal region of the cadavers. The mean pullout force was measured as 47.5 N ± 5.0.
Conclusions: We report a feasibility study for the application of novel needle-based colpopexy under CT-image guidance. Further clinical studies are required to implement this method in clinical settings and to demonstrate its safety and effectiveness compared with conventional surgical procedures.
Keywords: CT; Cadaver; Image-guided intervention; Medical device; Minimally invasive procedure; Pelvic organ prolapse.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical/Institutional Review Board Approval: Catholic University of Korea Seoul St. Mary’s Hospital IRB Review Result Notice [Form Number: MC22EIGC0074]. Conflicts of Interest: B.C., K.H.L., and H.C. have no conflicts of interest to declare. K.T.B. and C.K. submitted a provisional patent application.
Figures




References
-
- Schulten SFM, Detollenaere RJ, Stekelenburg J, IntHout J, Kluivers KB, van Eijndhoven HWF. Sacrospinous hysteropexy versus vaginal hysterectomy with uterosacral ligament suspension in women with uterine prolapse stage 2 or higher: observational follow-up of a multicentre randomised trial. BMJ. 2019;366:l5149. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
