

Hemodynamic effects of adjunct arginine vasopressin to norepinephrine in septic shock: insights from a prospective multicenter registry study
- PMID: 40299108
- PMCID: PMC12040798
- DOI: 10.1186/s13613-025-01472-w
Hemodynamic effects of adjunct arginine vasopressin to norepinephrine in septic shock: insights from a prospective multicenter registry study
Abstract
Background: The Surviving Sepsis Campaign guidelines suggest adding arginine vasopressin (AVP) when norepinephrine (NE) doses reach 0.25-0.50 µg/kg/min in septic shock patients. However, relying solely on a NE threshold has limitations, as other factors may be valuable in guiding AVP therapy during septic shock. Therefore, we aimed to identify additional patient characteristics associated with AVP hemodynamic responsiveness.
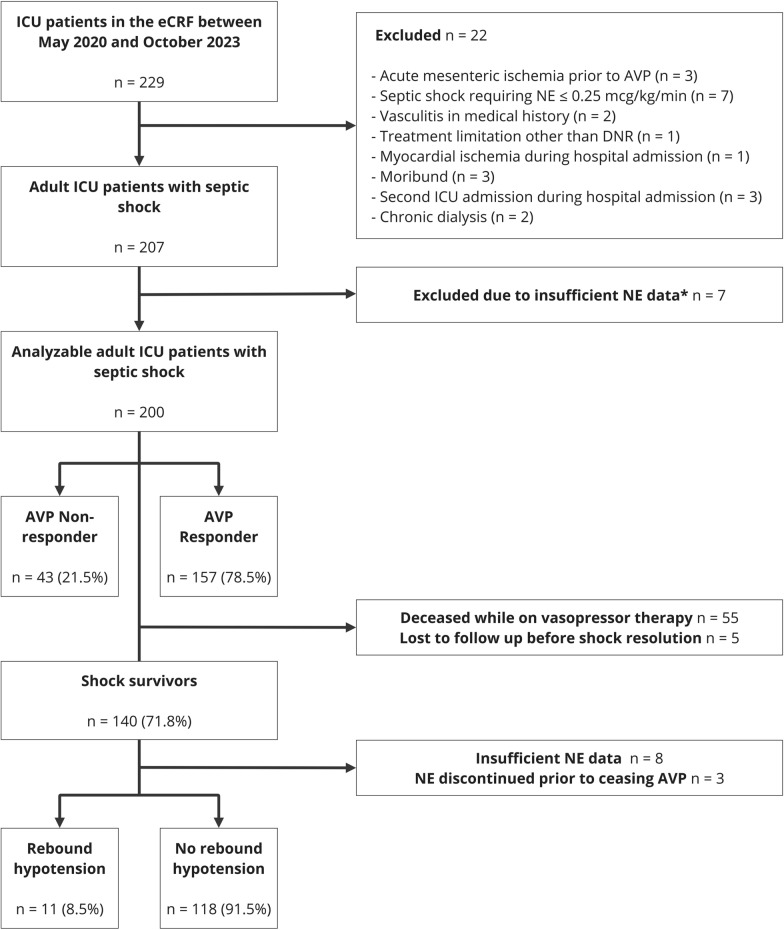
Methods: A multicenter, prospective, observational study was conducted among adult ICU patients who met the predefined criteria for septic shock (not reaching the individual target mean arterial pressure despite adequate fluid resuscitation and NE base dose > 0.25 µg/kg/min) and received AVP therapy. AVP hemodynamic responsiveness was the primary study outcome, defined as stabilization or decrease of NE infusion rate two hours after initiating AVP. Secondary outcomes included shock duration and rebound hypotension following termination of AVP infusion. Univariate and multivariable regression analyses were performed to detect associations between characteristics and outcomes.
Results: Between May 2020 and October 2023, 200 septic shock patients originating from 11 different ICUs were included. Of these, 153 (79%) met the definition for AVP hemodynamic responsiveness. Obesity and hyperlactatemia was negatively associated with AVP-response (adjusted Odds Ratio [aOR] 0.30, 95%CI 0.14-0.65 and aOR 0.86, 95%CI 0.75-0.99, respectively), while a NE infusion rate ≥ 0.30 µg/kg/min showed positive odds of AVP response (aOR 2.33, 95%CI 1.06-5.14). Incidence of new-onset atrial fibrillation was lower in AVP responders than non-responders (4% vs. 14%, p = 0.013). Higher body mass index (BMI) , NE infusion rate and duration prior to AVP initiation was associated with longer shock duration (aOR 1.06, 95%CI 1.02-1.11, aOR 1.12, 95%CI 1.01-1.25, and 1.01 95% CI 1.00-1.03, respectively), while higher pH associated with lower likelihood of prolonged shock (aOR 0.80, 95%CI 0.64-0.99). Rebound hypotension occurred in 9% when AVP was terminated, and AVP duration > 24 h was negatively associated with rebound hypotension (OR 0.22, 95%CI 0.05-0.85).
Conclusions: Arterial lactate, pH, BMI, and NE duration and dose were associated with AVP responsiveness and shock duration during septic shock, and rebound hypotension occurred in 9% during recovery. Our findings suggest that beyond NE thresholds, specific factors could be considered to optimize adjunctive AVP therapy in septic shock patients.
Keywords: Arginine vasopressin; Body mass index; Intensive care unit; Norepinephrine; Sepsis; Shock.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study received a waiver from the Dutch 'Medical Research Involving Human Subjects Act' from the medical ethical committee of Wageningen University and Research on December 20, 2020. Informed consent was obtained from each subject or, when applicable, from a legal representative, next of kin, or proxy in accordance to local protocols. Consent for publication: Not applicable. Competing interests: MM reported receiving honoraria and travel expenses from AOP pharma. AvZ reported receiving honoraria for advisory board meetings, lectures, research, and travel expenses from AOP Pharma, Abbott, Baxter, Cardinal Health, Danone-Nutricia, DIM3, Dutch Medical Food, Fresenius Kabi, GE Healthcare, InBody, Mermaid, Rousselot, and Lyric. The other authors have nothing to declare.
Figures

References
-
- Antonucci E, Polo T, Giovini M, Girardis M, Martin-Loeches I, Nielsen ND, et al. Refractory septic shock and alternative wordings: a systematic review of literature. J Crit Care. 2023;75: 154258. - PubMed
-
- Wieruszewski ED, Jones GM, Samarin MJ, Kimmons LA. Predictors of dysrhythmias with norepinephrine use in septic shock. J Crit Care. 2021;61:133–7. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
