

Serum Levels of Irisin Are Positively Associated with Improved Cardiac Function in Patients with Heart Failure with Reduced Ejection Fraction
- PMID: 40299414
- PMCID: PMC12024550
- DOI: 10.3390/biomedicines13040866
Serum Levels of Irisin Are Positively Associated with Improved Cardiac Function in Patients with Heart Failure with Reduced Ejection Fraction
Abstract
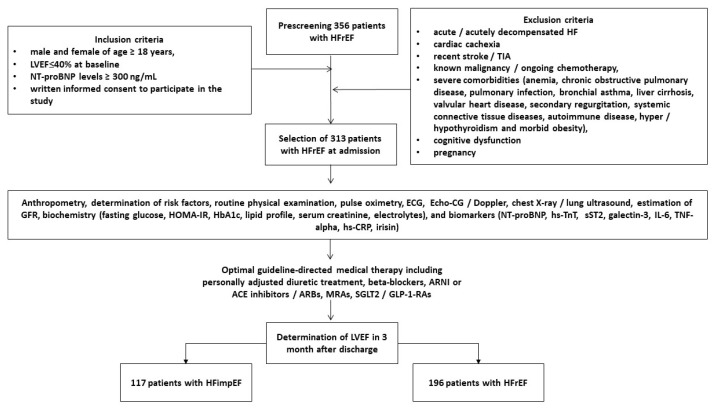
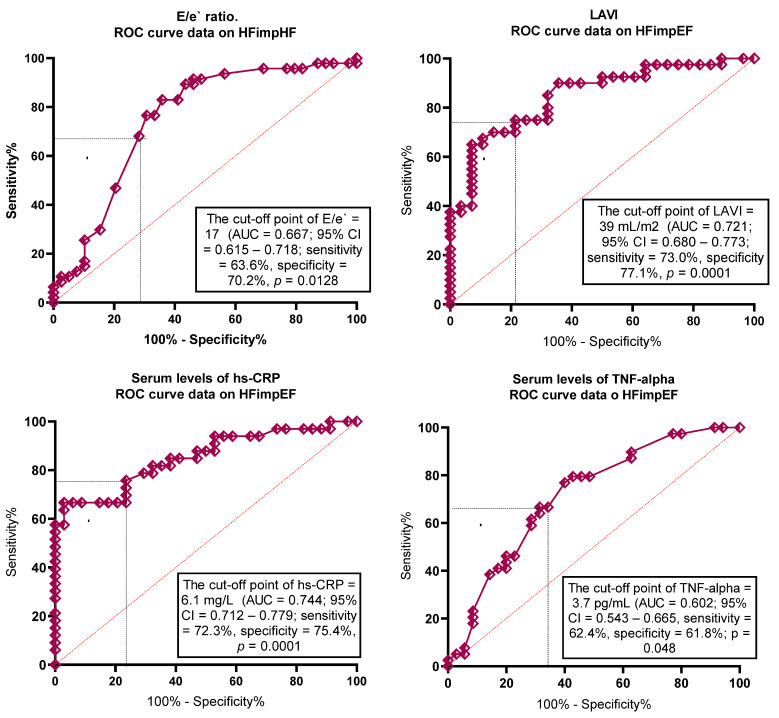
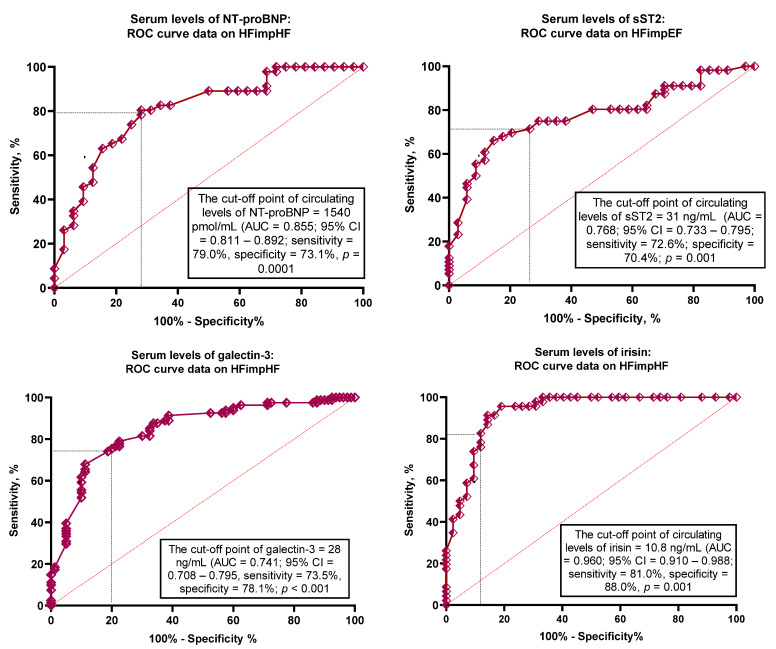
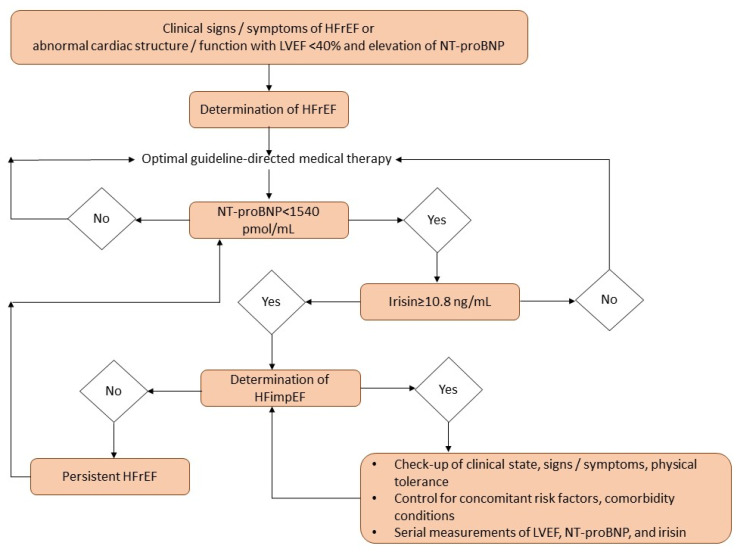
Background: The purpose of the study is to investigate a possible predictive value of irisin for improved left ventricular (LV) ejection fraction (EF) in discharged patients with known heart failure with reduced ejection fraction (HFrEF). Methods: We included in the study 313 patients who were discharged with HFrEF (at admission, LVEF ≤ 40%) and monitored for 3 months. HF with improved LVEF (HFimpEF) was characterized as a >40% increase in LVEF on transthoracic B-mode echocardiography within 3 months of follow-up. Circulating biomarkers including NT-proBNP and irisin were detected at baseline and after 3 months of observation. By the third month, 117 (37.4%) patients had HFimpEF, whereas 196 individuals were categorized as having persistent HFrEF. Results: We found that HFimpEF was related to lower LV end-diastolic dimensions and concentrations of NT-proBNP and higher left atrial volume index (LAVI) and irisin concentrations than those with persistent HFrEF. The most balanced cut-offs of irisin and NT-proBNP concentrations (improved LVEF versus non-improved LVEF) were 10.8 ng/mL and 1540 pmol/L, respectively. Multivariate regression analysis showed that atrial fibrillation (odds ratio [OR] = 0.95; p = 0.010), LAVI < 39 mL/m2 (OR = 1.23; p = 0.001), irisin levels ≥ 10.8 ng/mL (OR = 1.73; p = 0.001), and NT-proBNP < 1540 pmol/mL (OR = 1.47; p = 0.001) independently predicted HFimpEF. The discriminative ability of irisin ≥ 10.8 ng/mL was better than NT-proBNP < 1540 pmol/mL; the predictive ability of irisin alone was not improved by the combined model (irisin added to NT-proBNP). Conclusions: serum irisin ≥ 10.8 ng/mL predicted HFimpEF independently of natriuretic peptide in HFrEF patients.
Keywords: biomarkers; cardiac function; heart failure; improved ejection fraction; irisin; natriuretic peptides.
Conflict of interest statement
Author Oleksandr O. Berezin was employed by Luzerner Psychiatrie AG. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Left atrial volume and left ventricular mass indices in heart failure with preserved and reduced ejection fraction.ESC Heart Fail. 2021 Aug;8(4):2458-2466. doi: 10.1002/ehf2.13366. Epub 2021 Jun 4. ESC Heart Fail. 2021. PMID: 34085774 Free PMC article.
-
Tissue inhibitor of metalloproteinase (TIMP)-1 predicts failure of recovery of ejection fraction in acute heart failure with reduced ejection fraction.Open Heart. 2024 Sep 25;11(2):e002770. doi: 10.1136/openhrt-2024-002770. Open Heart. 2024. PMID: 39322629 Free PMC article.
-
Irisin Predicts Poor Clinical Outcomes in Patients with Heart Failure with Preserved Ejection Fraction and Low Levels of N-Terminal Pro-B-Type Natriuretic Peptide.Biomolecules. 2024 Dec 17;14(12):1615. doi: 10.3390/biom14121615. Biomolecules. 2024. PMID: 39766322 Free PMC article.
-
Predictive value of serum irisin for chronic heart failure in patients with type 2 diabetes mellitus.Mol Biomed. 2022 Nov 9;3(1):34. doi: 10.1186/s43556-022-00096-x. Mol Biomed. 2022. PMID: 36350412 Free PMC article.
-
Quality of life in patients with heart failure and improved ejection fraction: one-year changes and prognosis.ESC Heart Fail. 2022 Dec;9(6):3804-3813. doi: 10.1002/ehf2.14098. Epub 2022 Aug 2. ESC Heart Fail. 2022. PMID: 35916351 Free PMC article. Review.
References
-
- Savarese G., Becher P.M., Lund L.H., Seferovic P., Rosano G.M.C., Coats A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023;118:3272–3287. doi: 10.1093/cvr/cvac013. Erratum in Cardiovasc. Res. 2023, 119, 1453. https://doi.org/10.1093/cvr/cvad026 . - DOI - PubMed
-
- Bozkurt B., Ahmad T., Alexander K.M., Baker W.L., Bosak K., Breathett K., Fonarow G.C., Heidenreich P., Ho J.E., Hsich E., et al. Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. J. Card. Fail. 2023;29:1412–1451. doi: 10.1016/j.cardfail.2023.07.006. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
