

Fungal Pulmonary Coinfections in COVID-19: Microbiological Assessment, Inflammatory Profiles, and Clinical Outcomes
- PMID: 40299432
- PMCID: PMC12024551
- DOI: 10.3390/biomedicines13040864
Fungal Pulmonary Coinfections in COVID-19: Microbiological Assessment, Inflammatory Profiles, and Clinical Outcomes
Abstract
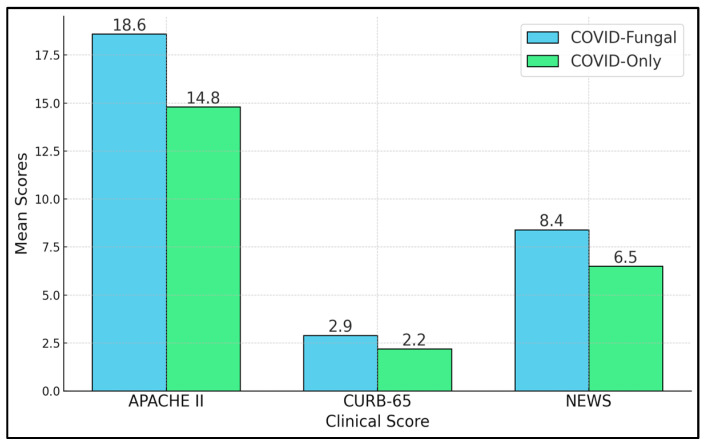
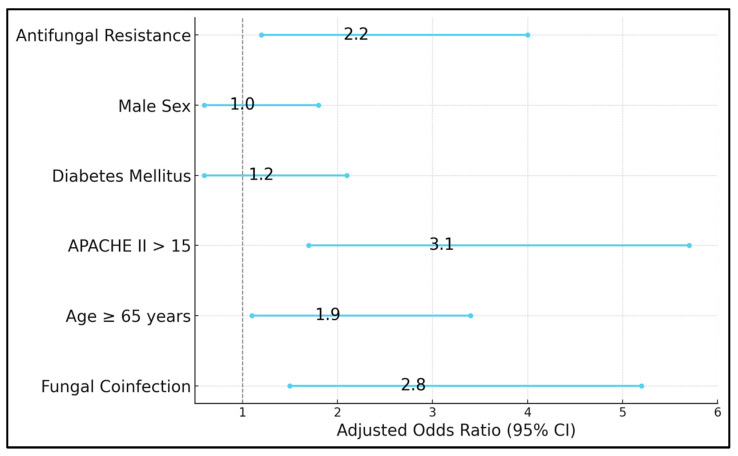
Background and Objectives: Secondary pulmonary fungal infections in coronavirus disease 2019 (COVID-19) remain underexplored despite emerging reports linking them to heightened morbidity. Comorbidities, steroid use, and prolonged hospital stays can predispose patients to opportunistic fungi. This study aimed to evaluate the impact of fungal coinfection on inflammatory markers, disease severity, antifungal resistance profiles, and outcomes in hospitalized COVID-19 patients. Methods: This retrospective observational study enrolled 280 adults (≥18 years) with real-time polymerase chain reaction (RT-PCR)-confirmed COVID-19 admitted to a tertiary care center (January 2023-December 2024). Patients were divided into a COVID-19-only group (n = 216) and a COVID-fungal group (n = 64) based on bronchoalveolar lavage, sputum, and/or blood culture positivity for fungal pathogens. Inflammatory markers (C-reactive protein (CRP), procalcitonin, the neutrophil-to-lymphocyte ratio, and the systemic immune inflammation index) and severity scores (Acute Physiology and Chronic Health Evaluation II, CURB-65 score, and the National Early Warning Score) were measured. We assessed antifungal susceptibilities and recorded ICU admissions, ventilation, hospital length of stay, and mortality. Results:Aspergillus fumigatus (31.3%), Candida albicans (28.1%), Cryptococcus neoformans (7.8%), Pneumocystis jirovecii (6.3%), and Mucorales (6.3%) dominated; Candida glabrata, Candida tropicalis, and mixed infections were also noted. Multidrug-resistant (MDR) isolates or resistance to triazoles occurred in 25.0% of cultures. The COVID-19-fungal group showed significantly higher CRP (85.7 vs. 71.6 mg/L, p < 0.001), procalcitonin (2.4 vs. 1.3 ng/mL, p < 0.001), and APACHE II scores (18.6 vs. 14.8, p < 0.001). intensive-care unit admissions (39.1% vs. 19.9%, p = 0.004) and mechanical ventilation (26.6% vs. 10.2%, p = 0.01) were more frequent with fungal coinfection. Mortality trended at a higher rate (15.6% vs. 7.4%, p = 0.06). Conclusions: Pulmonary fungal coinfections intensify the inflammatory milieu, elevate severity scores, and lead to more frequent ICU-level interventions in COVID-19 patients. Early identification, guided by culture-based and molecular diagnostics, alongside prompt antifungal therapy, could mitigate adverse outcomes. These findings underscore the critical need for proactive fungal surveillance and rigorous stewardship in managing severe COVID-19 pneumonia.
Keywords: COVID-19; antifungal resistance; clinical outcomes; disease severity; pulmonary fungal infections.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
