

Radiological approach to metatarsalgia in current practice: an educational review
- PMID: 40301191
- PMCID: PMC12041408
- DOI: 10.1186/s13244-025-01945-3
Radiological approach to metatarsalgia in current practice: an educational review
Abstract
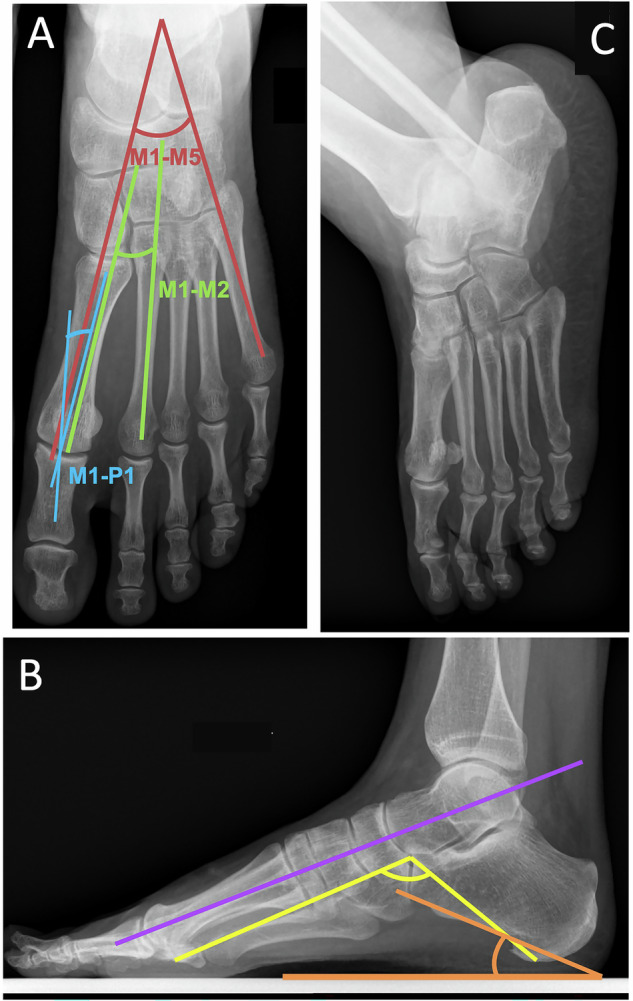
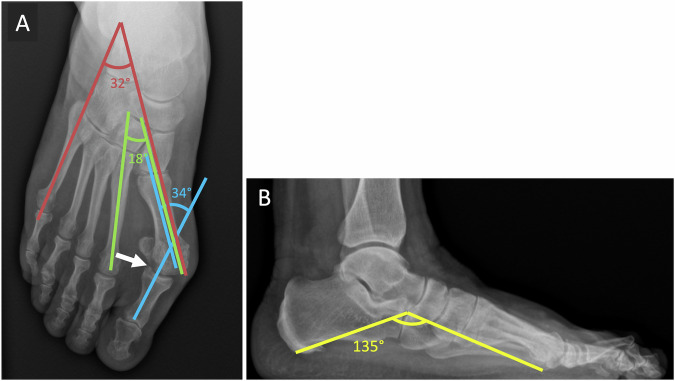
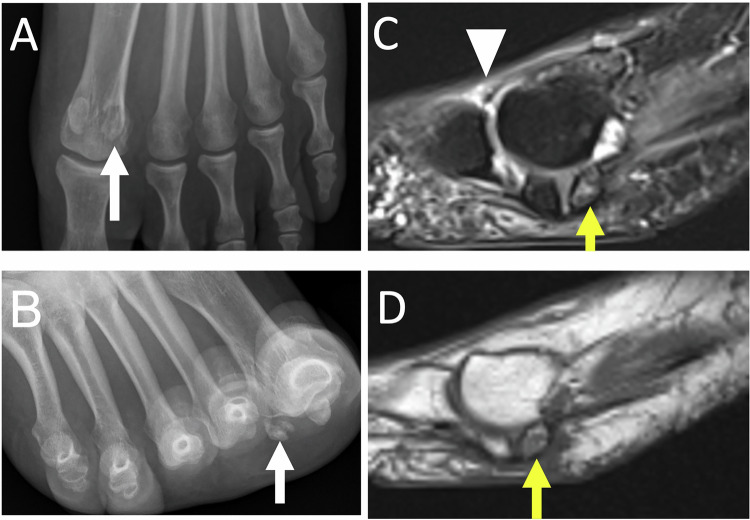
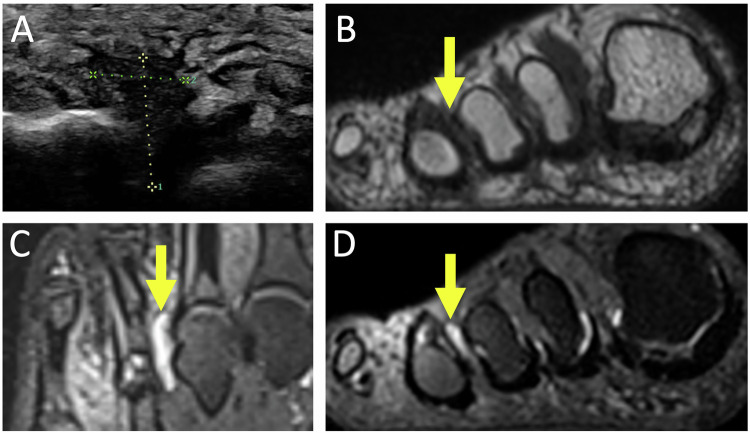
Metatarsalgia, characterized by forefoot pain, is frequent and is primarily due to foot static disorders. Initial evaluation with weight-bearing radiographs is essential, allowing precise analysis of the architecture of the foot. Ultrasound is useful for soft tissue and tendon examination and provides the best clinical correlation. Computed Tomography provides detailed bone assessment and is helpful for pre-operative planning. Magnetic Resonance Imaging is the gold standard modality, offering superior soft tissue contrast. The common causes of metatarsalgia include hallux pathologies (hallux valgus, hallux rigidus, and sesamoid issues), bursitis (intermetatarsal and subcapitellar), Morton's neuroma, second ray syndrome, stress fractures, and systemic pathologies affecting the foot. Combining clinical and imaging data is crucial for accurate diagnosis and effective management of metatarsalgia. Post-traumatic causes of metatarsalgia are beyond the scope of this article and will not be described. CRITICAL RELEVANCE STATEMENT: Metatarsalgia, the pain of the forefoot, necessitates accurate imaging for diagnosis and management. This review critically assesses imaging techniques and diagnostic approaches, aiming to enhance radiological practice and support effective therapeutic decision-making. KEY POINTS: Metatarsalgia commonly results from foot static disorders, requiring weight-bearing radiographs for assessment. MRI is often the gold standard examination, but ultrasound is complementary, allowing for a radioclinical approach with dynamic examinations. The radiologist is crucial in diagnosing metatarsalgia, providing essential imaging, and guiding treatment.
Keywords: Forefoot; MRI; Metatarsalgia; Radiograph; Ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: University Hospitals of Angers and Rennes guidelines do not require individual consent for the publication of images, as long as they are anonymized. Competing interests: The authors declare that they have no known competing interests.
Figures



References
-
- Guerini H, Morvan G, Mathieu P et al (2014) Métatarsalgies et imagerie: algorithme diagnostique. Rev Rhum Monogr 81:138–146
-
- Thomas JL, Kunkel MW, Lopez R, Sparks D (2006) Radiographic values of the adult foot in a standardized population. J Foot Ankle Surg 45:3–12 - PubMed
-
- Joong MA, El-Khoury GY (2007) Radiologic evaluation of chronic foot pain. Am Fam Phys 76:975–983 - PubMed
-
- Djian A, Annonier C, Denis A, Baudoin P(1968) Radiopodometry (principles and results)] J Radiol Electrol Med Nucl 49:769–772 - PubMed
LinkOut - more resources
Full Text Sources
