

Broad rim lesions are a new pathological and imaging biomarker for rapid disease progression in multiple sclerosis
- PMID: 40301560
- PMCID: PMC12176629
- DOI: 10.1038/s41591-025-03625-7
Broad rim lesions are a new pathological and imaging biomarker for rapid disease progression in multiple sclerosis
Abstract
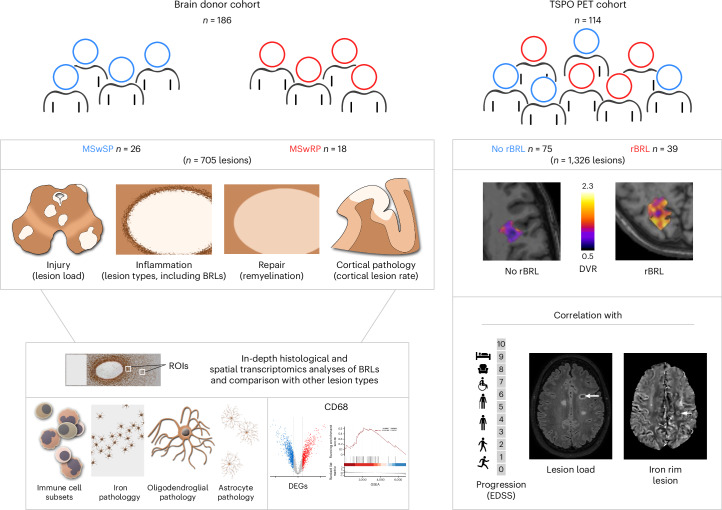
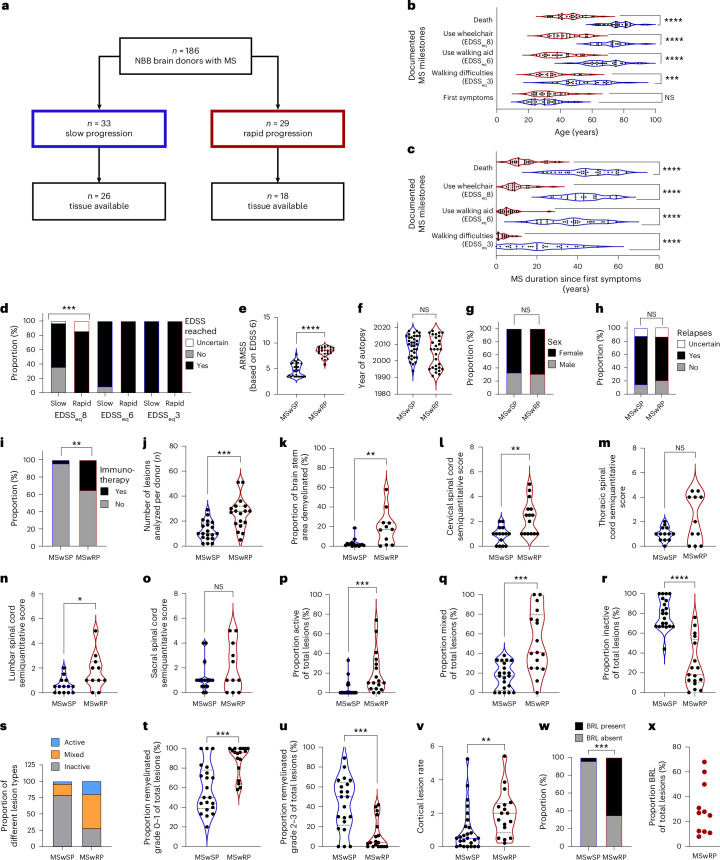
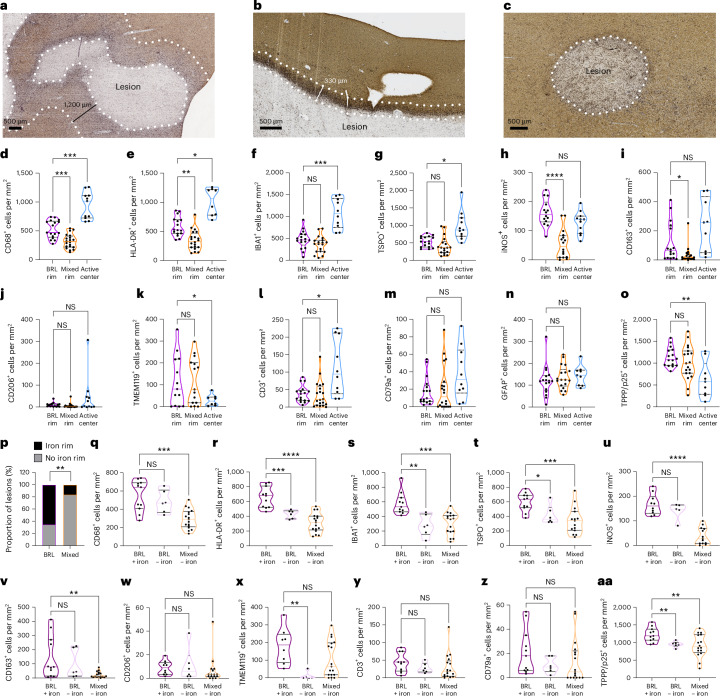
Current multiple sclerosis (MS) treatments reduce relapse activity but have limited impact on disease progression. Clinical trials targeting progression often fail because of insufficient understanding of its underlying mechanisms. This study analyzed a clinically well-characterized MS autopsy cohort from the Netherland Brain Bank (186 individuals) from which we selected donors exhibiting opposite disease trajectories of slow versus rapid progression. We performed extensive unbiased histology and spatial transcriptomics, which unveiled a distinct MS lesion type marked by an extensive myeloid cell rim with cellular and transcriptional signatures of innate immune activation, inflammatory cytokine production, unfolded protein response and apoptosis. Presence of this particular lesion type was linked to rapid disease progression. An independent translocator protein 18-kDa positron emission tomography study (114 individuals) validates the association between lesions with a broad myeloid cell rim and disease progression in individuals with MS. Our findings offer crucial insights into the mechanisms behind MS progression, identifying broad rim lesions as a biomarker for rapid disease progression and potentially guiding patient selection for future therapeutic trials targeting central nervous system intrinsic inflammation.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: L.K. receives research support from the DFG, the Interdisciplinary Center for Clinical Research (IZKF) Münster, the National MS Society, Biogen, Novartis and Merck Serono. She received compensation for serving on scientific advisory boards and speaker honoraria from Alexion, Amgen, Argenx, Bayer, Biogen, Bristol Myers Squibb, Grifols, Hexal, Horizon, Janssen, Merck Serono, Novartis, Roche, Sandoz, Sanofi, Santhera, Teva and Viatris. J.S. receives research support from Roche, Siemens Healthineers, Hansa Biopharma, Stichting MS research, Stichting klimmen tegen MS (MOVES inspiration grant), Nationaal MS fonds and the Erasmus Foundation, and received speaker honoraria or consultancy fees from Biogen, Merck, Novartis, Roche and Sanofi. He serves on the steering committee of the International Progressive MS Alliance, the scientific advisory board of Stichting MS research and several committees of the Dutch Society for Neurology. J.L. received speaker honoraria from Merck and Sanofi. H.W. receives research support from the DFG, the Deutsche Myasthenie Gesellschaft, the European Union, Alexion, Amicus Therapeutics, Argenx, Biogen, CSL Behring, F. Hoffmann-La Roche, Genzyme, Merck KGaA, Novartis, Roche and UCB Biopharma, as well as speaker honoraria or consultancy fees from Alexion, Argenx, Argobio, AOCN, AstraZeneca, BGP Products Operations, Biogen, Bristol Myers Squibb, CEMCAT, Dianthus, EMD Serono, EPG Health/Medthority, Fondazione Cariplo, Genzyme, Idorsia, Immunic, Immunovant, INmune Bio Syneos Health, Kohlhammer, LTS, Lundbeck, Merck, MS at the Limits, Muna Therapeutics, Myrobalan Therapeutics, Neurodiem, NMSS, Novartis, Ology, PSL Group, Red Nucleus, Roche, Samsung, Sangamo, Sanofi, Springer, StreamedUp, the Swiss MS Society, Teladochealth, Toleranzia, Teva, UCB, Uvet, Viatris and WebMD global. He is a member of the scientific advisory boards of Alexion, Argenx, Biocryst, Bristol Myers Squibb, Cellerys, Galapagos, Janssen, Merck, Novartis, Sandoz-Hexal and uniQure biopharma. L.A. receives grants from the Research Council of Finland, the Aatos Erkko Foundation, the US National MS Society, Merck Serono and Sanofi. She has received speaker and advisory honoraria from Sanofi, Biogen, Novartis, Kiniksa, Continuum Therapeutics and Merck. I.H. has received compensation for serving on the scientific advisory board of Muna Therapeutics and serves on a speakers’ panel for Novartis. T.K. receives research funding from the DFG, IZKF Münster, the National MS Society, the German MS Society and Novartis. She has received compensation for serving on the scientific advisory boards of Novartis, Sanofi and Merck, and speaker honoraria from Novartis, Biogen, Sanofi and Roche. The other authors declare no competing interests.
Figures










References
-
- Stampanoni Bassi, M., Iezzi, E. & Centonze, D. Multiple sclerosis: inflammation, autoimmunity and plasticity. Handb. Clin. Neurol.184, 457–470 (2022). - PubMed
MeSH terms
Substances
Grants and funding
- CRC TR 128 B07/Deutsche Forschungsgemeinschaft (German Research Foundation)
- CRC TR128 A 08/Deutsche Forschungsgemeinschaft (German Research Foundation)
- TRR332 B02/Deutsche Forschungsgemeinschaft (German Research Foundation)
- CRC TR128 A09, A10, Z02/Deutsche Forschungsgemeinschaft (German Research Foundation)
- RFA180-2202-39141/National Multiple Sclerosis Society (National MS Society)
LinkOut - more resources
Full Text Sources
Medical
