

The potential for de-escalation radical surgery in women with stage IB2 cervical cancer (FIGO 2018): a multi-institutional experience of 63,926 cases over a 14-year period in China
- PMID: 40301786
- PMCID: PMC12039193
- DOI: 10.1186/s12893-025-02917-6
The potential for de-escalation radical surgery in women with stage IB2 cervical cancer (FIGO 2018): a multi-institutional experience of 63,926 cases over a 14-year period in China
Abstract
Objective: To compare the long-term survival outcomes, recurrence patterns and morbidity of type B and type C radical hysterectomy (RH) for stage IB2 cervical cancer (FIGO 2018).
Methods: Based on FOUR-C database, patients who underwent type B or C RH in 47 hospitals from 2004 to 2018 were reviewed. Univariate and multivariate analyses were performed to compare 5-year overall survival (OS) and recurrence-free survival (RFS), recurrence patterns and morbidity between the two groups after propensity score matching (PSM).
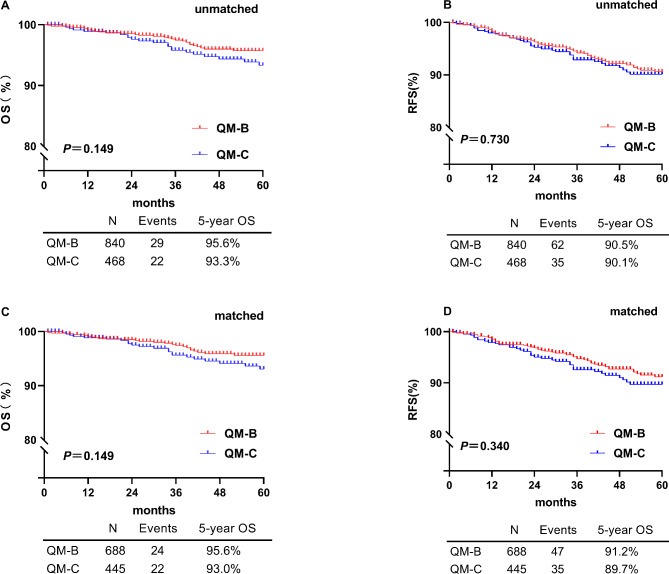
Results: A total of 1308 patients were enrolled in this study, 840 and 468 patients underwent type B and type C. There was no difference in 5-year survival outcomes between groups type B and type C, either before or after matching (OS: unmatched 95.6% vs. 93.3%, matched 95.6 vs. 93.0%, P>0.05; RFS: unmatched: 90.5% vs. 90.1%, matched: 91.2% vs. 89.7%, P>0.05). Type B group had a shorter operative time, less blood loss, earlier recovery of intestinal function, eariler removal of catheter and shorter hospitalization (P<0.01). Intraoperative complications were similar (0.1% vs. 0.2%, P>0.05), but postoperative complications occurred more frequently in the type C group (8.3% vs. 12.1%, P < 0.05), especially lymphocysts and urinary retention. The surgical dissection does not appear to influence tumor recurrences significantly (P>0.05).
Conclusions: For cervical cancer patients with stage IB2, type B RH demonstrated comparable long-term oncological outcomes and recurrence patterns to type C RH, while being associated with fewer intra-and postoperative complications. Type B RH is a feasible and appropriate surgical option, but the conclusions need to be confirmed by prospective studies.
Keywords: Cervical cancer; Complications; IB2; Recurrence; Type B; Type C.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical statement and consent to participate: The study was accomplished following the ethical principles according to the Declaration of Helsinki 1964. This retrospective study was approved by the Ethics Committee of the Nanfang Hospital of Southern Medical University (approval number NFEC-2017–135 and clinical trial number CHiCTR1800017778; International Clinical Trials Registry Platform Search Port, https://trialsearch.who.int/Trial2.aspx?TrialID=ChiCTR1800017778 , registered at 14/08/2018), who deemed that written informed consent was not necessarily due to the retrospective nature of the research and concealment of patient information. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Panici PB, Cutillo G, Angioli R. Modulation of surgery in early invasive cervical cancer. Crit Rev Oncol Hematol. 2003;48(3):263–70. - PubMed
-
- Benedet JL, Odicino F, Maisonneuve P, et al. Carcinoma of the cervix uteri. J Epidemiol Biostat. 2001;6(1):7–43. - PubMed
-
- Corrigendum to. Revised FIGO staging for carcinoma of the cervix uteri [Int J Gynecol Obstet 145(2019) 129–135]. Int J Gynaecol Obstet. 2019;147(2):279–280. - PubMed
Publication types
MeSH terms
Grants and funding
- 2014BAI05B03/The National Science and Technology Support Program of China
- 2014BAI05B03/The National Science and Technology Support Program of China
- 2015A030311024/The Natural Science Fund of Guangdong Province
- 2015A030311024/The Natural Science Fund of Guangdong Province
- 2023B03J0254/The Science and Technology Plan of Guangzhou
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
