

The burden and predictors of hospital-acquired infection in intensive care units across Sub-Sahara Africa: systematic review and metanalysis
- PMID: 40301793
- PMCID: PMC12042380
- DOI: 10.1186/s12879-025-11038-7
The burden and predictors of hospital-acquired infection in intensive care units across Sub-Sahara Africa: systematic review and metanalysis
Abstract
Background: Hospital-acquired infection (HAI) refers to an infection that occurs during hospitalization and typically manifests 48 h after admission. Evidence suggests that the prevalence of HAIs in Sub-Saharan Africa (SSA) is significantly higher compared to other regions. These infections remain a major concern in low-income countries, contributing to elevated morbidity and mortality rates. This study aimed to assess the burden and identify predictors of HAIs in intensive care units (ICUs) across SSA.
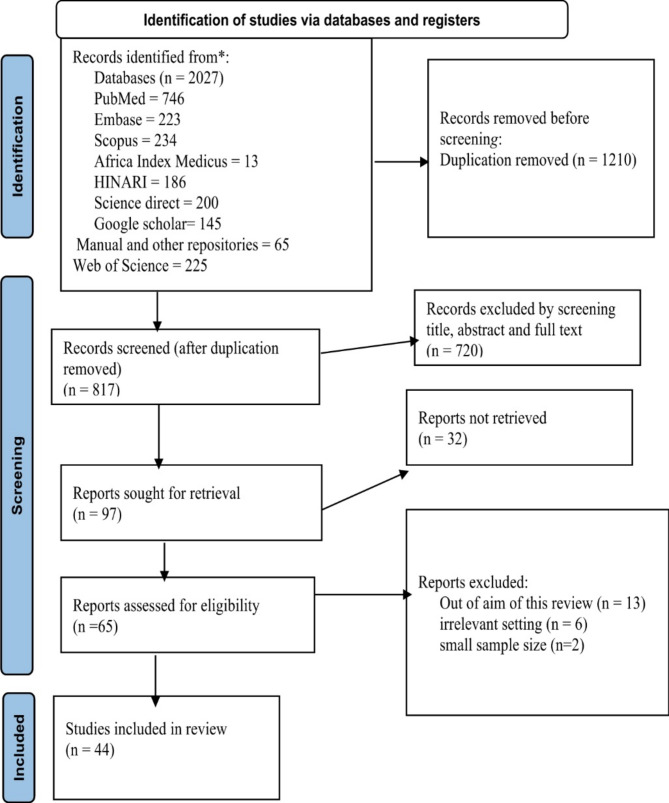
Methods: This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We searched PubMed, Scopus, Embase, Web of Science, Africa Index Medicus, ScienceDirect, HINARI, and Google Scholar to identify relevant studies published in English. This systematic review encompasses 44 articles published between 2003 and 2024, with the majority (22 articles) published recently between 2020 and 2024. The actual database search was conducted between January 1, 2025, and February 1, 2025. Articles irrelevant to this study's objectives, those without abstracts or full texts, unpublished reports, editorials, studies that did not clearly define outcomes, and studies written in languages other than English were excluded. The analysis was conducted using Stata version 17. The protocol was registered with PROSPERO under the registration number CRD 63,194,923,892. Quality assessment was performed using the Newcastle-Ottawa Scale, and data extraction followed the Joanna Briggs Institute methodology.
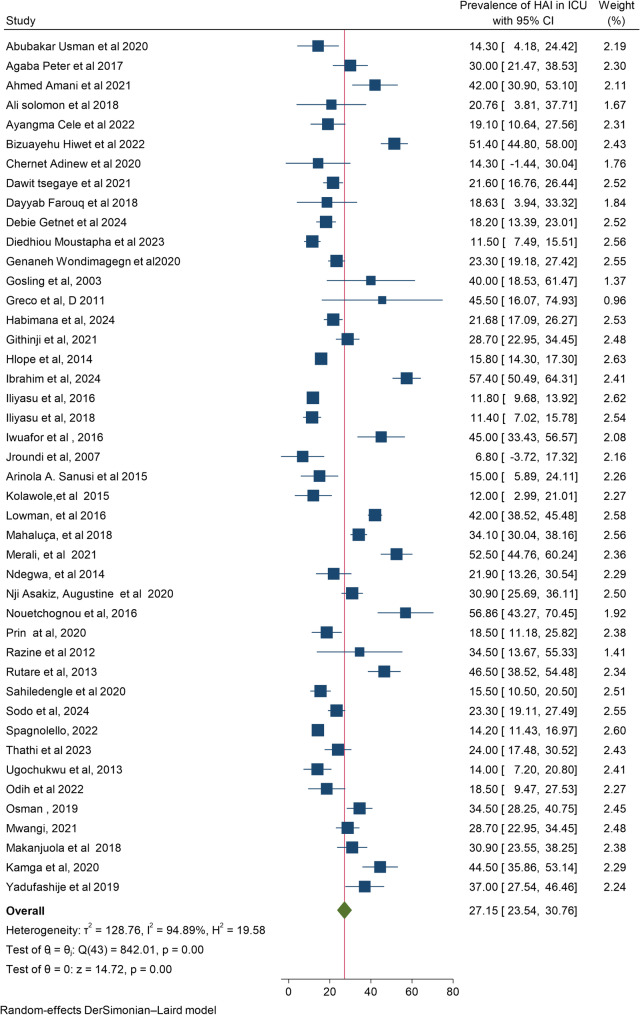
Results: A total of 44 primary samples were included in this meta-analysis. Using the random effect DerSimonian model, we showed that the pooled prevalence of hospital-acquired infections (HAIs) in intensive care units was 28.22% (95% CI: 23.61-32.81). Determinants of HAIs in the intensive care units included neonatal or advanced age (> 50 years), intubation, trauma, surgery, presence of comorbidities, catheterization, prolonged hospital stay, and HIV-positive status.
Conclusion and recommendations: Individuals in extreme age groups, those with chronic diseases or immunocompromised conditions, and patients with specific risk factors (e.g., catheterization, prolonged hospitalization) were more prone to HAIs. Strengthening the quality of care and implementing effective infection control measures are recommended to reduce the burden of healthcare-associated infections (HAIs) in sub-Saharan Africa.
Keywords: Hospital-acquired infection; Intensive care unit; Prevalence.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The ethical declaration is not applicable because this is a systematic review and meta-analysis. Consent to participate: Not applicable, it is a systematic review and metanalysis. Consent to publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Post-abortion family planning use and its determinants among women who received abortion care in sub-Saharan Africa: a systematic review and meta-analysis.Syst Rev. 2025 Jun 10;14(1):126. doi: 10.1186/s13643-025-02837-9. Syst Rev. 2025. PMID: 40495240 Free PMC article.
-
Mental health problems in pregnant and postpartum women living with HIV in sub-Saharan Africa: Systematic review and meta-analysis protocol.PLoS One. 2024 Oct 3;19(10):e0308810. doi: 10.1371/journal.pone.0308810. eCollection 2024. PLoS One. 2024. PMID: 39361676 Free PMC article.
-
Menstrual health needs and educational outcomes among adolescent girls living in countries in sub-Saharan Africa: systematic review protocol.BMJ Open. 2025 May 21;15(5):e094613. doi: 10.1136/bmjopen-2024-094613. BMJ Open. 2025. PMID: 40398941 Free PMC article.
-
The burden of hospital-acquired infections (HAI) in sub-Saharan Africa: a systematic review and meta-analysis.EClinicalMedicine. 2024 Apr 8;71:102571. doi: 10.1016/j.eclinm.2024.102571. eCollection 2024 May. EClinicalMedicine. 2024. PMID: 38606166 Free PMC article.
-
Obstetric admission and maternal mortality in the intensive care unit in Africa: A systematic review and meta-analysis.PLoS One. 2025 Apr 16;20(4):e0320254. doi: 10.1371/journal.pone.0320254. eCollection 2025. PLoS One. 2025. PMID: 40238732 Free PMC article.
References
-
- BIDERI JP, Rutayisire E, Ntakirutimana T, et al. Prevalence and factors associated with nosocomial infections in public hospitals of Rwanda. A Cross Sectional Study; 2024.
-
- Schreiber PW, Sax H, Wolfensberger A, et al. The preventable proportion of healthcare-associated infections 2005–2016: systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2018;39(11):1277–95. - PubMed
-
- Teerawattanapong N, Panich P, Kulpokin D, et al. A systematic review of the burden of multidrug-resistant healthcare-associated infections among intensive care unit patients in Southeast Asia: the rise of multidrug-resistant Acinetobacter baumannii. Infect Control Hosp Epidemiol. 2018;39(5):525–33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
