

Activity-based recovery training with spinal cord epidural stimulation improves standing performance in cervical spinal cord injury
- PMID: 40301929
- PMCID: PMC12042302
- DOI: 10.1186/s12984-025-01636-6
Activity-based recovery training with spinal cord epidural stimulation improves standing performance in cervical spinal cord injury
Abstract
Background: Individuals with a clinically complete spinal cord injury are unable to stand independently without external assistance. Studies have shown the combination of spinal cord epidural stimulation (scES) targeted for standing with activity-based recovery training (ABRT) can promote independence of standing in individuals with spinal cord injury. This cohort study aimed to assess the effects of stand-ABRT with scES in individuals with cervical chronic spinal cord injury. We evaluated the ability of these individuals to stand independently from physical assistance across multiple sessions.
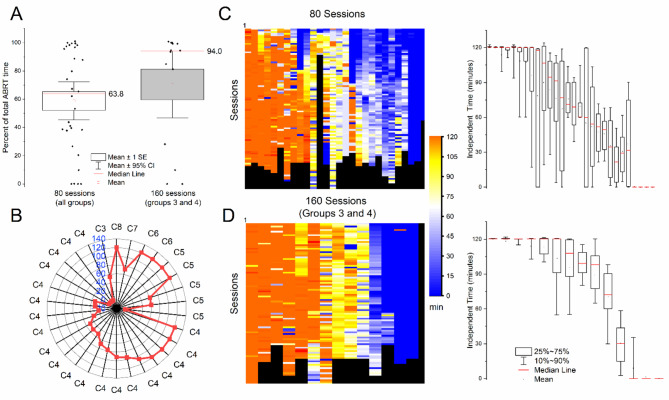
Methods: Thirty individuals participated in this study, all unable to stand independently at the start of the intervention. Individuals were participating in a randomized clinical trial and received stand-ABRT in addition to targeted cardiovascular scES or voluntary scES. During the standing intervention, participants were asked to stand 2 h a day, 5 days a week for 80 sessions (Groups 1 and 2) or 160 sessions (Groups 3 and 4).
Results: A total of 3,524 training days were considered for analysis. Group 1 had 507 days, group 2 with 578 days, and 1152 and 1269 days for groups 3 and 4 respectively. 71% of sessions reached the two-hour standing goal. All individuals achieved outcomes of lower limb independent extension with spinal cord epidural stimulation, with a wide range throughout a training day. Sixteen participants achieved unassisted hip extension while maintaining unassisted bilateral knee and trunk extension. Participants receiving initial voluntary scES training performed better in unassisted bilateral knee and trunk extension than those receiving initial cardiovascular scES. The lower-limb standing activation pattern changes were consistent with the greater standing independence observed by all groups.
Conclusions: Individuals with chronic cervical spinal cord injury were able to achieve various levels of extension without manual assistance during standing with balance assist following stand-ABRT with scES. These results provide evidence that scES modulates network excitability of the injured spinal cord to allow for the integration of afferent and supraspinal descending input to promote standing in individuals with spinal cord injury.
Trial registration: The study was registered on Clinical Trials.gov (NCT03364660) prior to subject enrollment.
Keywords: Cervical spinal cord injury; Epidural spinal stimulation; Independence; Rehabilitation; Standing.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Institutional Review Boad of the University of Louisville approved the study protocol (16–0179 and approved on 10/19/2017). All participants provided written informed consent according to the Declaration of Helsinki. Consent for publication: Research participants involved in the videos and images provided additional consent for publication. Competing interests: The authors declare no competing interests.
Figures






References
-
- Singh R, Rohilla RK, Saini G, Kaur K. Longitudinal study of body composition in spinal cord injury patients. Indian J Orthop [Internet]. 2014;48(2):168–77. Available from: https://www.ncbi.nlm.nih.gov/pubmed/24741139 - PMC - PubMed
-
- Castro MJ, Apple DF Jr., Staron RS, Campos GE, Dudley GA. Influence of complete spinal cord injury on skeletal muscle within 6 mo of injury. JApplPhysiol. 1999;86(1):350–8. - PubMed
-
- Cragg JJ, Noonan VK, Dvorak M, Krassioukov A, Mancini GB, Borisoff JF. Spinal cord injury and type 2 diabetes: Results from a population health survey. Neurology [Internet]. 2013; Available from: http://www.ncbi.nlm.nih.gov/pubmed/24153440 - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
