

HPV Genotype, AGC Categories, and Age-Stratified Immediate Prevalence of Precancers and Cancers in Women with Atypical Glandular Cells with or without Concurrent Squamous Abnormal Cytology
- PMID: 40302806
- PMCID: PMC12036100
- DOI: 10.7150/jca.105805
HPV Genotype, AGC Categories, and Age-Stratified Immediate Prevalence of Precancers and Cancers in Women with Atypical Glandular Cells with or without Concurrent Squamous Abnormal Cytology
Abstract
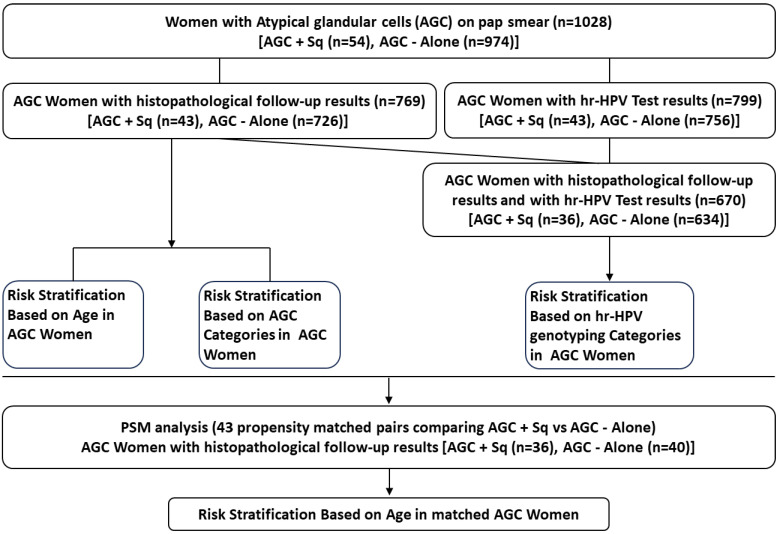
Objectives: Limited data exists on Papanicolaou (Pap) tests involving atypical glandular cells (AGC) with or without concurrent squamous cell abnormalities (Sq), hindering the reproducibility of results. This study aims to stratify the risk of precancers and cancers based on distinct high-risk human papillomavirus (hrHPV) genotyping, AGC categories, and age groups among women with AGC with or without concurrent squamous cell abnormalities. Methods: This retrospective analysis examined Pap smear patient data from January 2019 to December 2023, including 54 AGC + Sq cases and 974 cases with AGC-Alone. Among these, 799 patients (including 43 AGC + Sq cases and 756 AGC-Alone cases) had HPV testing results, and 769 (including 43 AGC + Sq cases and 726 AGC-Alone cases) had subsequent histological follow-up data. Results: In the total cohort, 5.25% (54 cases) were AGC + Sq, and 94.75% (974 cases) were AGC-Alone. The detection rates of high-grade glandular lesions (AIS+/AEH+) and adenocarcinoma (AC) were significantly higher in AGC patients over 65 years compared to other age groups (p = 0.000444 and p < 0.0001, respectively), while no significant differences were observed for high-grade squamous lesions (HSIL+) (p = 0.791) or squamous carcinoma (SCC) (p = 0.909). The prevalence of AIS+/AEH+ was significantly higher in HPV-16 (28.6%) and HPV-18 (50.0%) positive groups compared to the HPV-negative (10.4%) and other hrHPV types positive groups (6.3%) (p < 0.0001). Notably, the AGC + Sq group exhibited a higher prevalence of isolated squamous lesions, as well as glandular lesions with concurrent squamous involvement, compared to the AGC-Alone group (p = 0.001). Additionally, increased AC risk was observed in older AGC + Sq women at the 50-year cutoff, although no significant association was found between HPV genotype and immediate histology in the AGC + Sq group. Conclusions: A comprehensive approach that incorporates cytological results, hrHPV status, and age offers more effective stratification of AGC patients, leading to more precise management. While hrHPV testing and age provide valuable insights, relying solely on hrHPV results for triaging AGC + Sq cases is inadequate.
Keywords: Atypical glandular cells; Papanicolaou (Pap) test; coexisting glandular and squamous cells abnormalities; histological follow-up; risk stratification.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures


References
-
- Islami F, Fedewa SA, Jemal A. Trends in cervical cancer incidence rates by age, race/ethnicity, histological subtype, and stage at diagnosis in the United States. Preventive medicine. 2019;123:316–323. - PubMed
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA: a cancer journal for clinicians. 2021;71(1):7–33. - PubMed
-
- Kalir T, Simsir A, Demopoulos HB, Demopoulos RI. Obstacles to the early detection of endocervical adenocarcinoma. International journal of gynecological pathology: official journal of the International Society of Gynecological Pathologists. 2005;24(4):399–403. - PubMed
-
- Harbhajanka A, Dahoud W, Michael CW. Can we predict histological outcome of distinctive cohorts of patients with glandular cell abnormalities on ThinPrep Papanicolaou testing based on human papillomavirus status, age, and associated squamous abnormalities? Diagnostic cytopathology. 2019;47(10):1028–1036. - PubMed
-
- Khor LY, Abdul-Karim FW, Bruening AE, Weber Noffsinger DK, Booth CN. Papanicolaou tests with coexisting squamous and glandular abnormalities. Cancer cytopathology. 2014;122(8):620–626. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
