

The Use of Novosorb Biodegradable Temporizing Matrix for Reconstruction in Head and Neck Cancer: A Simple Answer to a Complex Problem
- PMID: 40303322
- PMCID: PMC12040060
- DOI: 10.1097/GOX.0000000000006702
The Use of Novosorb Biodegradable Temporizing Matrix for Reconstruction in Head and Neck Cancer: A Simple Answer to a Complex Problem
Abstract
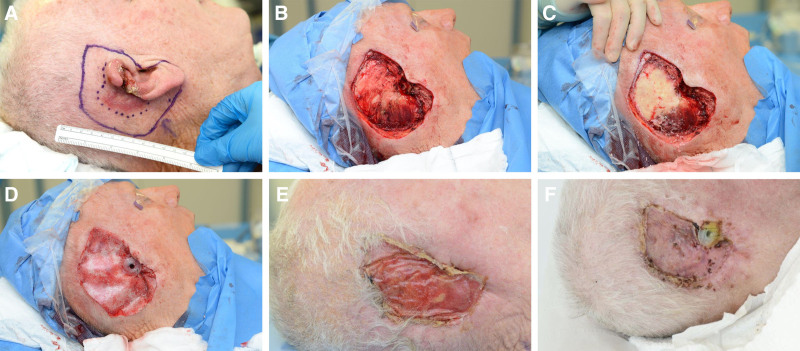
Background: Skin cancer defects in the head and neck can pose a reconstructive challenge. We aimed to evaluate our experience of Novosorb biodegradable temporizing matrix (BTM) in reconstructing complex defects in the head and neck region.
Methods: Assessment of all patients where BTM was used for head and neck skin cancer reconstruction was undertaken at our facility. This included tumor type; defect size; second-stage reconstruction (SSR) method; and complications, including failure.
Results: Fifty-four patients were identified with 63 lesions reconstructed with BTM. The mean age was 79. Histology was squamous/basosquamous carcinoma in 40 cases (63%), basal cell carcinoma in 15 cases (24%), and melanoma in 3 cases (5%). The anatomical region reconstructed was the scalp in 46 cases (73%) and the nose in 13 cases (21%). Mean maximum defect diameter was 67 mm. In 27 cases (43%), a previous wide local excision demonstrated an involved or close (<1 mm) margin. BTM was applied to burred bone in 24 of these cases (89%). SSR occurred via use of split-thickness skin graft (68%), full-thickness skin graft (14%), or via secondary intention (17%). One (1%) patient died before SSR, unrelated to BTM. SSR was carried out at a mean of 51 days. Five areas of 63 (8%) experienced a failure to fully heal, identified as due to recurrent or residual disease, causing wound breakdown. No significant infections were observed.
Conclusions: BTM offers a safe, reliable option for complex head and neck cancer reconstruction, particularly in patients unable to undergo more complex procedures.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article.
Figures




References
-
- Ahmed-Nusrath A. Anaesthesia for head and neck cancer surgery. BJA Educ. 2017;17:383–389.
-
- Ang KK. Multidisciplinary management of locally advanced SCCHN: optimizing treatment outcomes. Oncologist. 2008;13:899–910. - PubMed
-
- Eytan DF, Blackford AL, Eisele DW, et al. Prevalence of comorbidities among older head and neck cancer survivors in the United States. Otolaryngol Head Neck Surg. 2019;160:85–92. - PubMed
-
- Hu X, Zeng G, Zhou Y, et al. Reconstruction of skin defects on the mid and lower face using expanded flap in the neck. J Craniofac Surg. 2017;28:e137–e141. - PubMed
LinkOut - more resources
Full Text Sources