

Barriers to the implementation of large-scale electronic health record systems in primary healthcare centers: a mixed-methods study in Saudi Arabia
- PMID: 40303363
- PMCID: PMC12037483
- DOI: 10.3389/fmed.2025.1516714
Barriers to the implementation of large-scale electronic health record systems in primary healthcare centers: a mixed-methods study in Saudi Arabia
Abstract
Background: In the past two decades, policymakers have increasingly prioritized the integration of technology to enhance healthcare quality and efficiency. However, nearly half of these initiatives have failed to achieve their intended objectives due to various challenges, including financial constraints and implementation complexities. The Saudi Ministry of Health (MoH) launched a nationwide initiative to implement an Electronic Health Record System (EHRS) across approximately 2,200 Primary Healthcare Centers (PHCs). However, previous attempts at deployment encountered significant obstacles, leading to project failure. Key challenges identified by the MoH included inadequate infrastructure, limited connectivity, and lack of system interoperability.
Aim: To explore the key barriers hindering the effective implementation of EHRS in PHCs in Saudi Arabia, with a focus on technical, organizational, and user-related challenges.
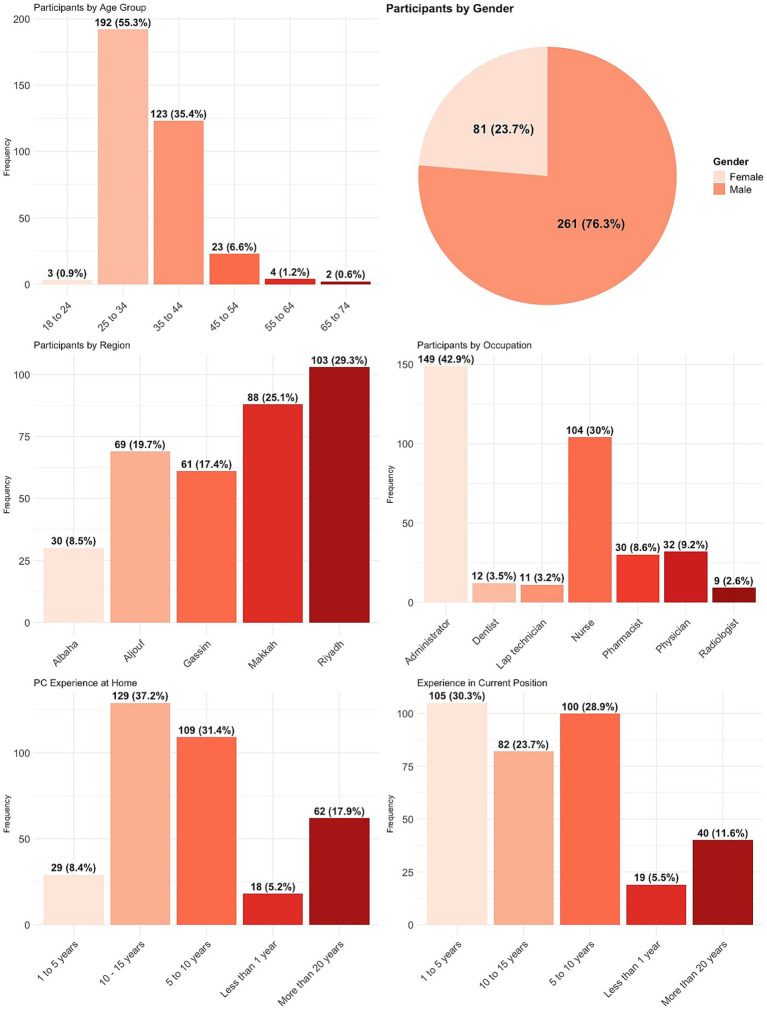
Method: This study adopted a mixed methods approach using an exploratory sequential design to capture both strategic and operational perspectives on EHRS implementation. The qualitative phase involved semi-structured interviews with 14 key informants from the MoH who were directly involved in the EHRS deployment, aiming to identify structural and policy-related barriers. The quantitative phase consisted of an online survey completed by 351 PHC practitioners to assess user-level challenges, including system usability, training adequacy, and technical support availability. This sequential approach ensured that the survey was informed by the insights gained from the qualitative phase.
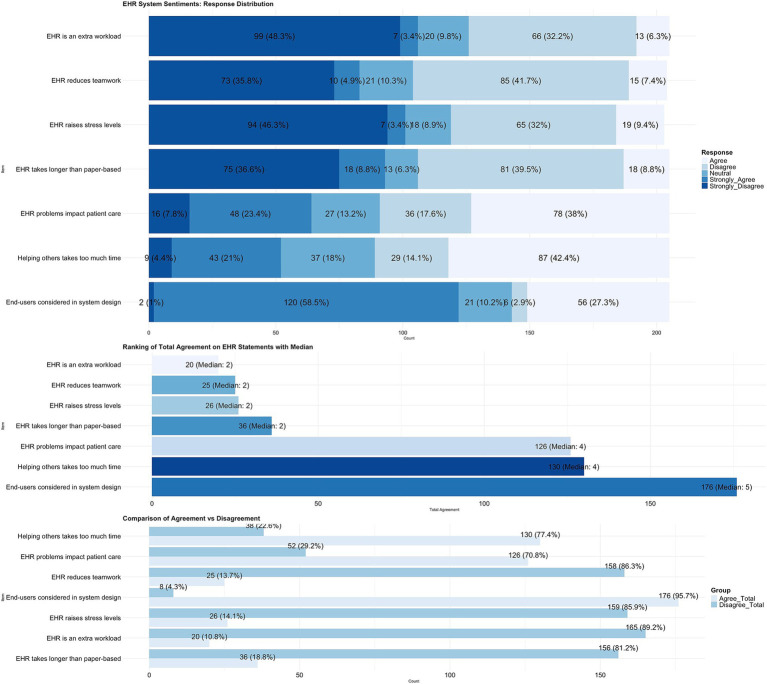
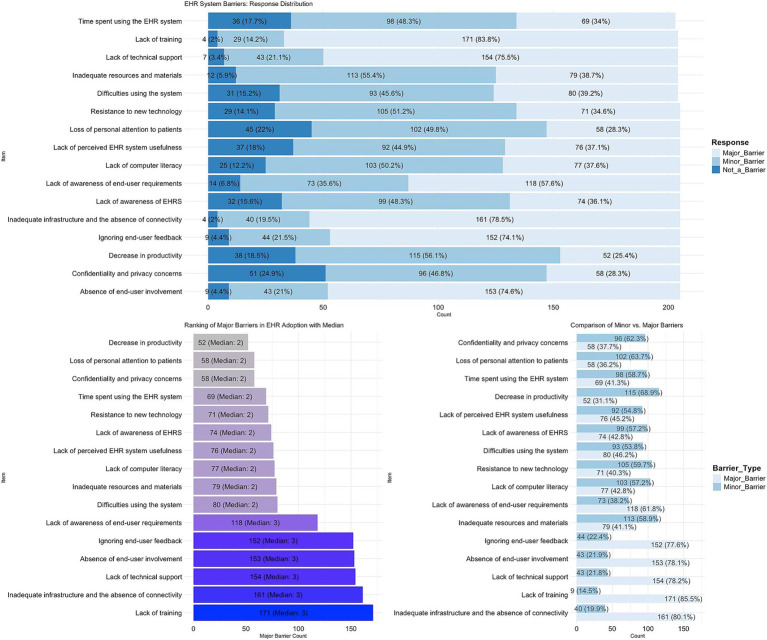
Results: Findings from both phases revealed multiple barriers affecting EHRS implementation. Key challenges included the large-scale nature of the project, resistance to change, insufficient training, lack of technical support, poor system interoperability, geographical limitations, and inadequate user engagement. Additionally, unclear software selection criteria contributed to integration difficulties. To address these barriers, the study proposes several strategies, including collaborating with telecom providers to improve connectivity, implementing a phased regional deployment strategy, and enhancing training and technical support frameworks.
Conclusion: The study highlights insufficient connectivity, inadequate technical support, and high turnover in key leadership positions as major contributors to previous implementation failures. Notably, training and ongoing support emerged as critical obstacles, whereas concerns related to privacy and confidentiality were found to be less significant. To ensure successful EHRS adoption, decision-makers must allocate sufficient resources for software selection, infrastructure improvements, workforce training, and continuous technical support. This study fills a research gap by providing evidence-based recommendations for optimizing large-scale EHRS implementation in healthcare settings, particularly in resource-constrained environments.
Keywords: Saudi Arabia; barriers; electronic health records; large-scale IT projects; mixed methods; primary healthcare centers; questionnaire; semi-structured interviews.
Copyright © 2025 Alzghaibi and Hutchings.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lennon MR, Bouamrane MM, Devlin AM, O'Connor S, O'Donnell C, Chetty U, et al. Readiness for delivering digital health at scale: lessons from a longitudinal qualitative evaluation of a National Digital Health Innovation Program in the United Kingdom. J Med Internet Res. (2017) 19:e42. doi: 10.2196/jmir.6900, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous