

The value of multi-sequence magnetic resonance imaging and whole-tumor apparent diffusion coefficient histogram analysis in differentiating p53 abnormal from non-p53 abnormal endometrial carcinoma
- PMID: 40304002
- PMCID: PMC12039310
- DOI: 10.3389/fonc.2025.1565152
The value of multi-sequence magnetic resonance imaging and whole-tumor apparent diffusion coefficient histogram analysis in differentiating p53 abnormal from non-p53 abnormal endometrial carcinoma
Abstract
Objective: To investigate the utility of multi-sequence magnetic resonance imaging (MRI) and whole-tumor apparent diffusion coefficient (ADC) histogram metrics in preoperatively differentiating p53 abnormal (p53abn) from non-p53abn endometrial carcinoma (EC).
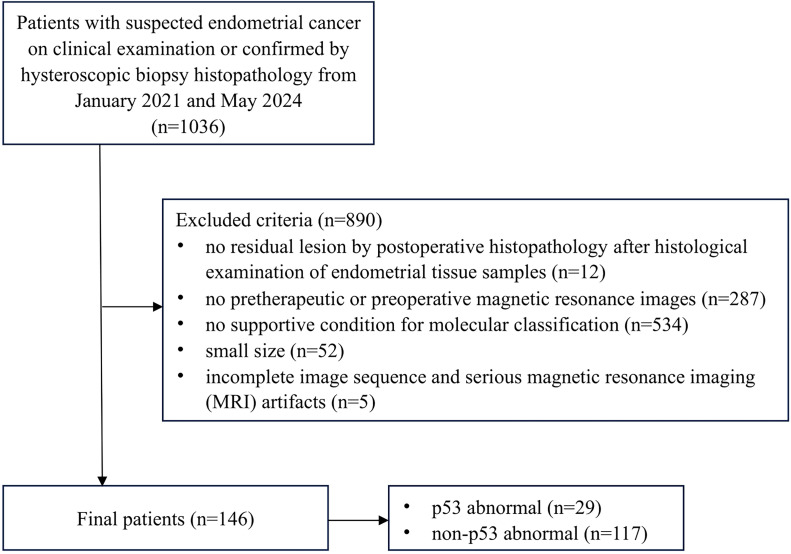
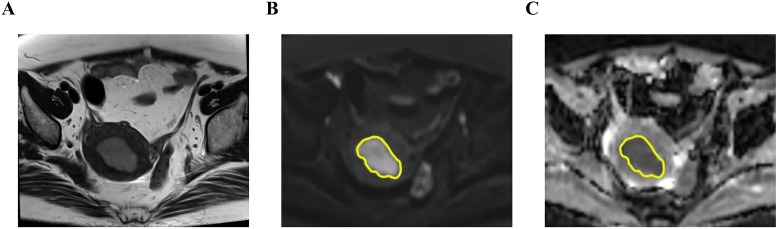
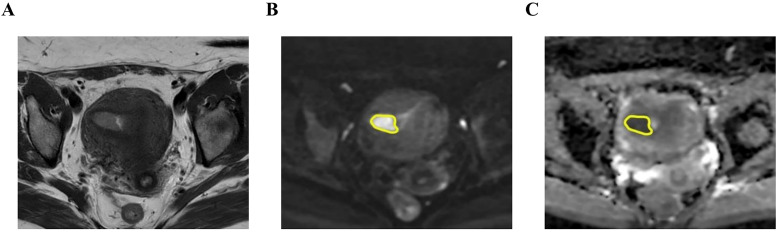
Methods: This retrospective study included 146 EC patients (29 p53abn cases and 117 non-p53abn cases) who underwent preoperative MRI scans. MRI features were analyzed. Whole-tumor ADC histogram analysis was conducted by delineating regions of interest (ROIs) on diffusion-weighted imaging (DWI) scans. Receiver operating characteristic (ROC) curve analysis with the area under the curve (AUC) was used for diagnostic performance evaluation.
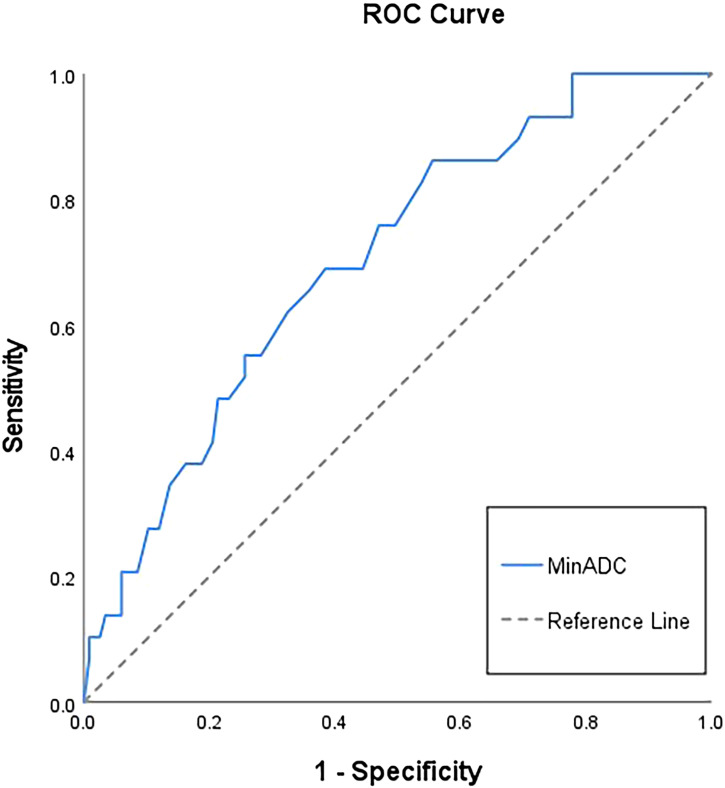
Results: Extrauterine extension (p=0.004) and lymphadenopathy (p=0.005) were more frequently observed in p53abn EC compared to non-p53abn EC. p53abn EC exhibited significantly lower value of minADC (p=0.001), meanADC (p=0.005), P10 (p=0.009), P50 (p=0.007), and P90 (p=0.013) ADC and higher value of kurtosis (p=0.008), compared to non-p53abn EC. MinADC demonstrated the highest discrimination ability in differentiating p53abn from non-p53abn EC [AUC 0.70(0.60;0.80)].
Conclusion: Preoperative multi-sequence MRI findings and whole-tumor ADC histogram metrics are conducive to differentiating p53abn from non-p53abn EC.
Keywords: diffusion-weighted imaging; endometrial cancer; histogram analysis; magnetic resonance imaging; p53.
Copyright © 2025 Sun, Zhang, Wang, Zhang and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The value of multimodal functional magnetic resonance imaging in differentiating p53abn from p53wt endometrial carcinoma.Acta Radiol. 2023 Nov;64(11):2948-2956. doi: 10.1177/02841851231198911. Epub 2023 Sep 3. Acta Radiol. 2023. PMID: 37661630
-
Whole-tumor apparent diffusion coefficient histogram analysis for preoperative risk stratification in endometrial endometrioid adenocarcinoma.Int J Gynaecol Obstet. 2024 Mar;164(3):1174-1183. doi: 10.1002/ijgo.15226. Epub 2023 Nov 4. Int J Gynaecol Obstet. 2024. PMID: 37925611
-
Whole-lesion apparent diffusion coefficient (ADC) histogram as a quantitative biomarker to preoperatively differentiate stage IA endometrial carcinoma from benign endometrial lesions.BMC Med Imaging. 2022 Aug 8;22(1):139. doi: 10.1186/s12880-022-00864-9. BMC Med Imaging. 2022. PMID: 35941559 Free PMC article.
-
The role of volumetric ADC histogram analysis in preoperatively evaluating the tumour subtype and grade of endometrial cancer.Eur J Radiol. 2021 Jul;140:109745. doi: 10.1016/j.ejrad.2021.109745. Epub 2021 Apr 30. Eur J Radiol. 2021. PMID: 33962254
-
Application of Apparent Diffusion Coefficient Histogram Metrics for Differentiation of Pediatric Posterior Fossa Tumors : A Large Retrospective Study and Brief Review of Literature.Clin Neuroradiol. 2022 Dec;32(4):1097-1108. doi: 10.1007/s00062-022-01179-6. Epub 2022 Jun 8. Clin Neuroradiol. 2022. PMID: 35674799 Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous