

High-Dose Steroids, Treatment Escalation, and Healthcare Burden in Myasthenia Gravis: A US Claims-Based Cohort Study
- PMID: 40304847
- PMCID: PMC12089002
- DOI: 10.1007/s40120-025-00714-0
High-Dose Steroids, Treatment Escalation, and Healthcare Burden in Myasthenia Gravis: A US Claims-Based Cohort Study
Abstract
Introduction: Myasthenia gravis (MG) is a rare neuromuscular autoimmune disease, characterized by chronic, fluctuating muscle weakness and fatigability. Despite established therapies, many patients have inadequately controlled MG. We describe treatment escalation patterns and outcomes for patients with MG between 2010 and 2018.
Methods: We conducted a retrospective cohort analysis of medical and pharmacy claims data. Patients aged ≥ 18 years at MG diagnosis were included from two US Merative™ MarketScan® databases. MG treatment escalation was defined as an increase of the administered prednisolone-equivalent corticosteroid dose, use of add-on treatments, or treatment switches.
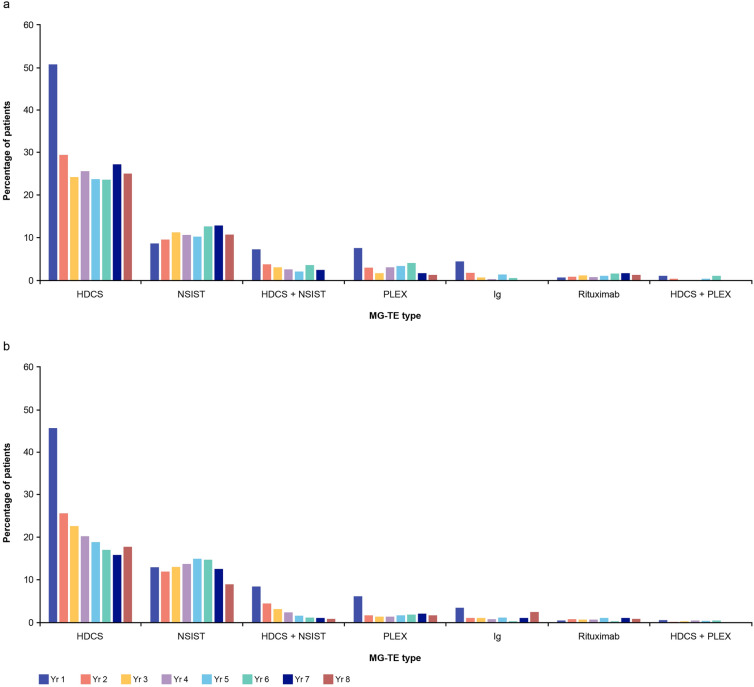
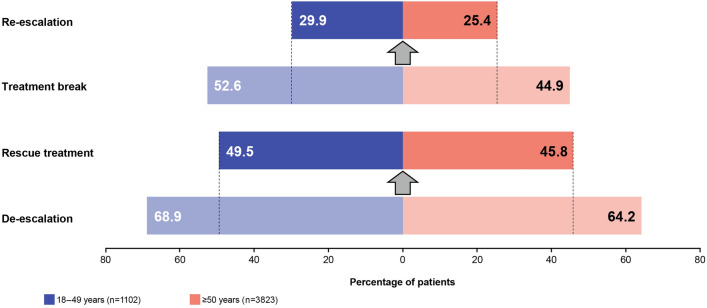
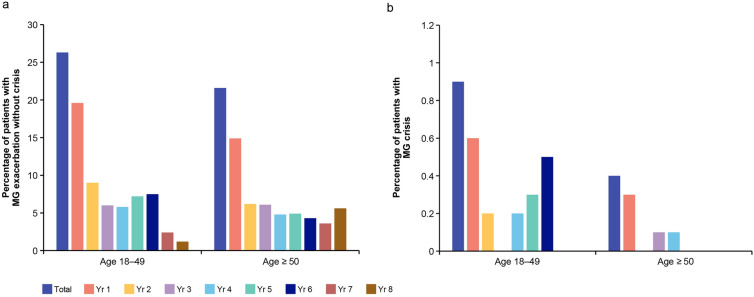
Results: The cohort included 4925 adults with newly diagnosed MG (1102 aged 18-49 and 3823 aged ≥ 50 at first MG diagnosis) from January 1, 2010 to December 31, 2018. Median follow-up was 30.0 months (18-49 group) and 27.5 months (≥ 50 group). Overall, 71.5% (3521/4925) of patients had ≥ 1 MG treatment escalation; escalation with high-dose corticosteroids was the most common type (64.8% [18-49 group] and 58.5% [≥ 50 group]). In the first year post-diagnosis, median (range) maximal daily prednisolone-equivalent corticosteroid dose was 40.0 (20.0-75.0) mg/day (18-49 group) and 40.0 (20.0-70.0) mg/day (≥ 50 group). Treatment breaks and de-escalation led to rescue treatment or treatment re-escalation in most patients. Exacerbations occurred in 26.3% (n = 290; 18-49 group) and 21.6% (n = 825; ≥ 50 group). Healthcare resource utilization (HCRU) and costs were highest in Year 1, with mean MG-related costs per patient between $24,982 (≥ 50 group) and $33,023 (18-49 group).
Conclusion: The study findings highlight that MG is inadequately controlled in a substantial proportion of patients despite conventional treatment and high reliance on corticosteroids. Earlier treatment with targeted therapies and improved safety profiles may reduce patient burden, HCRU, and costs.
Keywords: Cohort study; Corticosteroids; Healthcare costs; Healthcare resource utilization; Myasthenia gravis; Treatment escalation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Mar Pujades-Rodríguez, Jiachen Zhou and Thaïs Tarancón are employees and shareholders of UCB. Adam Jedrzejczyk and Olga Pilipczuk are contractors for UCB. Ethical Approval: We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines. UCB holds a license to use the data from both Merative™ MarketScan® research databases for research and publish the derived results. Because the databases used in this study consist of de-identified data compliant with the US Health Insurance Portability and Accountability Act of 1996, no ethics committee approval was required.
Figures
References
LinkOut - more resources
Full Text Sources
