

Comparative Analysis of Survival in Pulmonary Arterial Hypertension for Patients Treated with Selexipag in Clinical Practice (EXPOSURE Study)
- PMID: 40304966
- PMCID: PMC12173968
- DOI: 10.1007/s40801-025-00488-9
Comparative Analysis of Survival in Pulmonary Arterial Hypertension for Patients Treated with Selexipag in Clinical Practice (EXPOSURE Study)
Abstract
Background: In pulmonary arterial hypertension (PAH), comparative assessment of treatment effect on survival in randomized controlled settings of contemporary patients has not been feasible.
Objective: The aim of this study was to use EXPOSURE, the ongoing, real-world, post-authorization safety study, and commitment to the European Medicines Agency to perform pre-specified comparative survival analyses between patients that newly initiated selexipag versus other PAH-specific therapies by applying statistical methods to account for population differences.
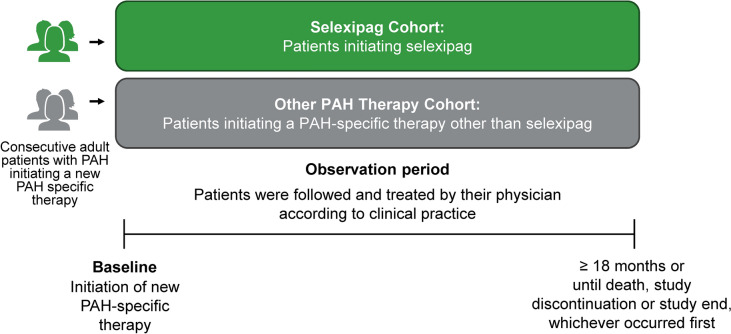
Methods: EXPOSURE (EUPAS19085) is an observational study comprising patients with PAH who initiated selexipag or other PAH-specific therapy. To balance characteristics of patients in the other PAH therapy cohort with the selexipag cohort at PAH therapy initiation (baseline), propensity score weighting was applied. Mortality rate ratios (MRRs) were calculated.
Results: 2014 patients were available for analysis. Prior to applying propensity score weighting, patients in the selexipag cohort were more likely to have longer time from diagnosis, less functional impairment, and treatment with combination background therapy versus the other PAH therapy cohort. Following weighting, baseline variables for both cohorts were well balanced. Weighted treatment exposure was 827.9 and 840.5 person-years for the selexipag and modelled other PAH therapy cohort, respectively. Weighted proportion of deaths was lower in the selexipag versus modelled other PAH therapy cohort; MRR showed a higher survival rate for selexipag-treated patients (MRR [95% confidence interval]: 0.55 [0.31-0.99]).
Conclusions: Survival analyses in EXPOSURE suggest a reduced risk of mortality among the cohort of patients newly initiated on selexipag compared with the modelled cohort newly initiated with other PAH-specific therapies. Further research is needed to confirm this observation.
Trial registry: Trial registration: EUPAS19085.
Plain language summary
Pulmonary arterial hypertension (PAH) is a rare and progressive disease characterized by high blood pressure in the blood vessels of the lungs. The rare and progressive nature of the disease makes measuring the effect of treatments on survival in randomized controlled trials challenging. To investigate this, we used real-world data from the EXPOSURE study (EUPAS19085), along with advanced statistical methods of modelling. Our observations indicate that the relative risk of dying was lower with selexipag treatment compared with other PAH therapies.EXPOSURE is a post-approval study required by the European Medicines Agency, aimed at collecting data on patients with PAH who are starting a new PAH treatment in medical clinics. We analyzed 2014 patients, divided into two groups: one that started treatment with selexipag (selexipag group) and another that started other PAH medication(s) (other PAH therapy group). At the start of treatment, patients in the selexipag group had been diagnosed with PAH for longer and showed less severe symptoms compared with the other PAH therapy group. They were also more likely to be on a combination of at least two different PAH medications at the time they started treatment with selexipag. Because of these differences, we used statistical modelling to balance patient characteristics at the start of treatment to be able to compare the medications. After balancing the groups, our data suggest a lower relative risk of dying with selexipag treatment compared with treatment with other PAH therapies.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Funding: This study was funded by Johnson & Johnson. Conflict of interest: Stefan Söderberg has received speaker and consultancy fees, and financial support for participation in scientific events from Johnson & Johnson and MSD. Pilar Escribano-Subias has received grants / research support from Ferrer and GlaxoSmithKline, consulting fees from Johnson & Johnson, Acceleron, Ferrer and MSD, payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing or educational events from Johnson & Johnson, MSD, Ferrer and AOT, has received support from Johnson & Johnson and MSD for attending meetings and/or travel, and has participated on a Data Safety Monitoring Board or Advisory Board for Johnson & Johnson, MSD, Ferrer, Gossamer, AOT, Acceleron and GlaxoSmithKline. Ciara Archey is an employee of Johnson & Johnson and has Johnson & Johnson shares. Audrey Muller is an employee of Johnson & Johnson and has Johnson & Johnson shares. Martina Fontana is an employee of Johnson & Johnson and has Johnson & Johnson shares. Tobias J. Lange has received speaker fees and/or consultancy fees and/or financial and non-financial support for participation in scientific events and/or participated on a Data Safety Monitoring Board or Advisory Board for Acceleron Pharma Inc, AOP orphan pharmaceuticals, Bayer, BMS, Böhringer Ingelheim, CGI medicare, Ferrer, Gossamer Bio, Johnson & Johnson, MSD, and Pfizer. Sean Gaine has had relations, such as funding, with the following subjects that have commercial interests in the pharmaceutical and medical field: Aerovate Therapeutics, Acceleron Pharma Inc, Altavant, Gossamer Bio, Johnson & Johnson, MSD and United Therapeutics. Availability of data and material: These data are not currently publicly available for sharing, requests for sharing can be sent to the corresponding author and will be evaluated on an individual basis. Ethics approval: The study was conducted in compliance with the Declaration of Helsinki and the protocol was approved at each study site (and at the national level in Sweden) by an Institutional Review Board or Independent Ethics Committee (Table S1, see ESM). The study was conducted in accordance with the International Society for Pharmacoepidemiology Guidelines for Good Pharmacoepidemiology Practices and the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance Guide on Methodological Standards in Pharmacoepidemiology. Consent to participate and for publication: Written informed consent was obtained for each patient for accessing and processing anonymized patient data and their use in scientific research. Code availability: Not applicable. Author contributions: Stefan Söderberg, Pilar Escribano-Subias, Ciara Archey, Tobias J. Lange and Sean Gaine contributed to the conceptualization, writing – original draft and writing – reviewing and editing. Audrey Muller contributed to the conceptualization, data curation, formal analysis, methodology, writing – original draft and writing – reviewing and editing of the manuscript. Martina Fontana contributed to the data curation, formal analysis, validation, writing – original draft and writing – reviewing and editing. All authors read and approved the final manuscript.
Figures

Similar articles
-
Macitentan and Tadalafil Combination Therapy in Patients with Pulmonary Arterial Hypertension and Cardiovascular Comorbidities: Real-World Evidence from OPUS and OrPHeUS.Adv Ther. 2025 Jul;42(7):3306-3333. doi: 10.1007/s12325-025-03180-0. Epub 2025 May 19. Adv Ther. 2025. PMID: 40388087 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
-
High Risk of Venous Thromboembolism With Aspirin Prophylaxis After THA for High-riding Developmental Dysplasia of the Hip: A Retrospective, Comparative Study.Clin Orthop Relat Res. 2025 Jun 9. doi: 10.1097/CORR.0000000000003482. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40536765
-
Molecular feature-based classification of retroperitoneal liposarcoma: a prospective cohort study.Elife. 2025 May 23;14:RP100887. doi: 10.7554/eLife.100887. Elife. 2025. PMID: 40407808 Free PMC article.
-
Prenatal administration of progestogens for preventing spontaneous preterm birth in women with a multiple pregnancy.Cochrane Database Syst Rev. 2019 Nov 20;2019(11):CD012024. doi: 10.1002/14651858.CD012024.pub3. Cochrane Database Syst Rev. 2019. PMID: 31745984 Free PMC article.
References
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–9. - PubMed
-
- Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987;107:216–23. - PubMed
-
- Boucly A, Savale L, Jaïs X, Bauer F, Bergot E, Bertoletti L, et al. Association between initial treatment strategy and long-term survival in pulmonary arterial hypertension. Am J Resp Crit Care. 2021;204:842–54. 10.1164/rccm.202009-3698OC. - PubMed
-
- NHS Digital. National audit of pulmonary hypertension. 13th Annual Report. https://files.digital.nhs.uk/36/B8B717/NAPH%2013AR%20-%20Main%20Report%2.... Accessed July 2023.
LinkOut - more resources
Full Text Sources
