

A Neuroimmune Modulator for Alcohol Use Disorder: A Randomized Clinical Trial
- PMID: 40305022
- PMCID: PMC12044506
- DOI: 10.1001/jamanetworkopen.2025.7523
A Neuroimmune Modulator for Alcohol Use Disorder: A Randomized Clinical Trial
Abstract
Importance: The neuroimmune system represents a promising target for novel medications for alcohol use disorder (AUD). Ibudilast is a neuroimmune modulator which selectively inhibits phosphodiesterases (PDE) 3, PDE4, PDE10, and PDE11, and macrophage migration inhibitory factor (MIF).
Objective: To test the efficacy of ibudilast for AUD compared with placebo.
Design, setting, and participants: This randomized clinical trial was a double-masked, phase 2 trial conducted at an academic research center between October 2018 and April 2023. Eligible participants were adults seeking treatment for moderate or severe AUD. After completing the 12-week treatment period, participants were followed up for an additional 4 weeks.
Interventions: Ibudilast taken twice daily in 50 mg doses for 12 weeks vs placebo.
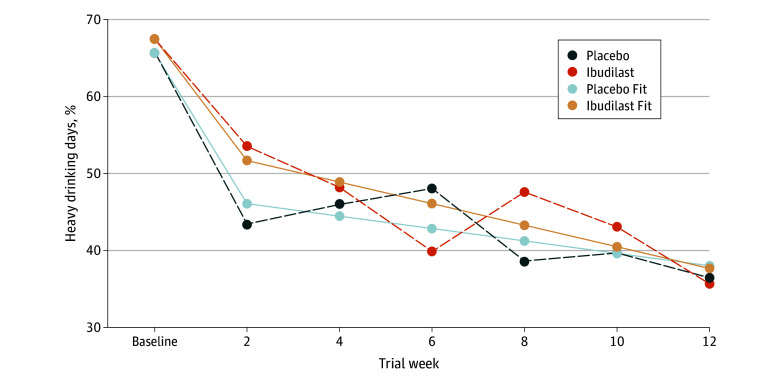
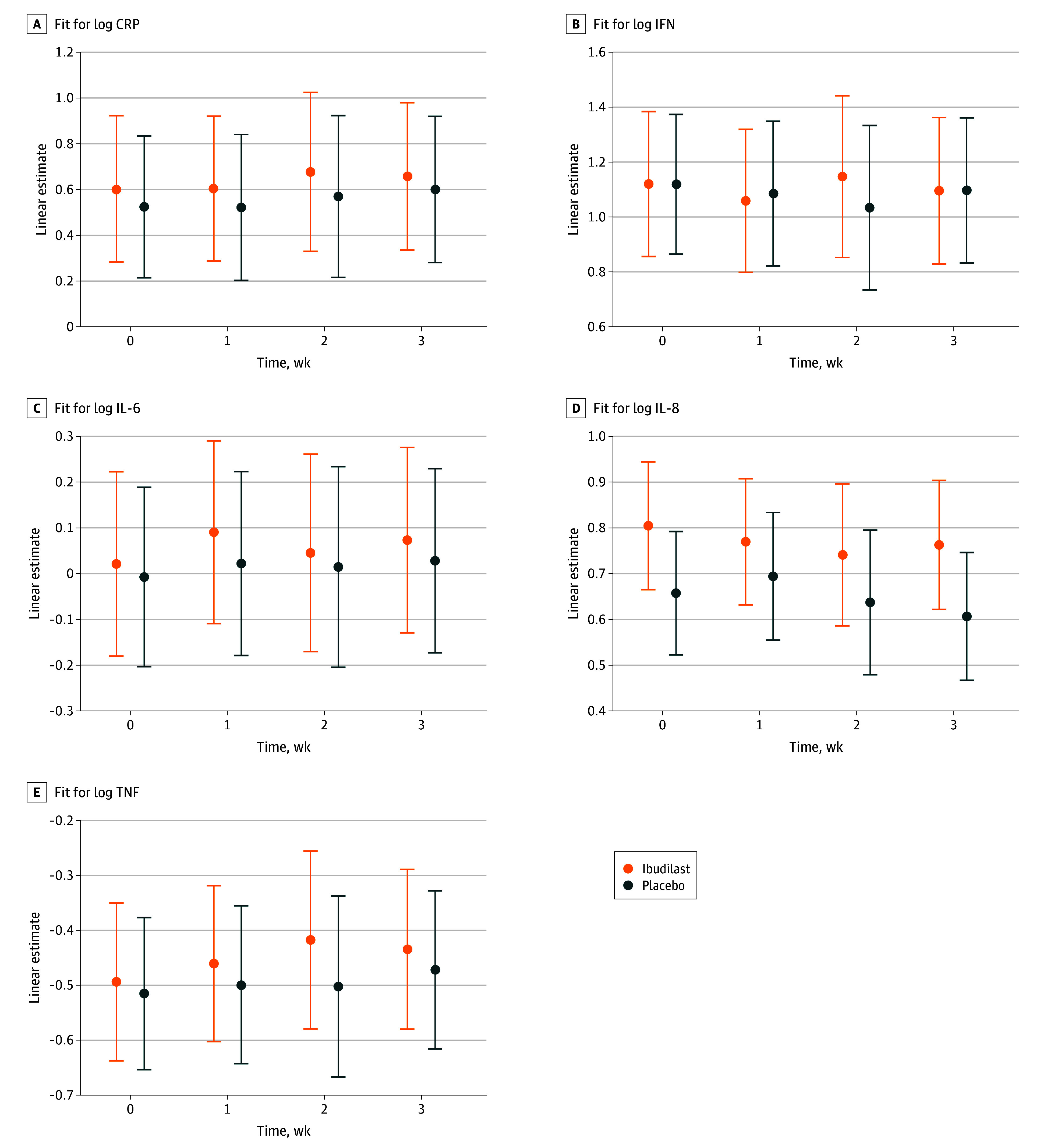
Main outcomes and measures: Percentage of heavy drinking days; secondary efficacy outcomes included drinks per day, drinks per drinking day, and percentage of days abstinent. Registered exploratory analyses tested whether the effects of ibudilast of drinking outcomes were moderated by baseline depressive symptomatology. Registered exploratory analyses also tested whether ibudilast reduced inflammation compared with placebo, as indicated by circulating levels of proinflammatory markers over the 12-week trial. Additionally, a post hoc exploratory analysis investigated whether sex moderated the effect of ibudilast on drinking outcomes. Data were analyzed between October 2018 and April 2023.
Results: A total of 102 participants were enrolled in the study (mean [SD] age, 44.3 [10.8] years; 61 male [59.8%]; 24 Black [23.5%], 32 Hispanic [31.4%], 52 White [51.0%]). Baseline demographic characteristics and alcohol use patterns did not significantly differ between the 2 medication conditions. There was no significant difference between ibudilast vs placebo on percentage of heavy drinking days (β = 0.06, SE = 0.08 [95% CI, -0.09 to 0.21]; P = .46). There were no significant differences between ibudilast vs placebo on registered secondary outcomes. There were no significant effects of ibudilast compared with placebo on peripheral markers of inflammation. Moderation analyses found that baseline depressive symptomology (time 2 for drinks per drinking day: β = 0.25, SE = 0.11 [95% CI, 0.03 to 0.48]; P = .03) and sex (β = -2.48, SE = 1.07 [95% CI, -4.59 to -0.37]; P = .02) may moderate the effects of ibudilast.
Conclusions and relevance: In this randomized clinical trial of ibudilast for the treatment of AUD, there was no support for the efficacy of ibudilast over placebo; additionally, no effect of ibudilast on markers of peripheral inflammation was observed. As novel treatments for AUD are developed for novel molecular targets, their effects may depend on mechanisms and moderators of efficacy.
Trial registration: ClinicalTrials.gov Identifier: NCT03594435.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
