

Functional characterization of the ATOH1 molecular subtype indicates a pro-metastatic role in small cell lung cancer
- PMID: 40305287
- PMCID: PMC12116416
- DOI: 10.1016/j.celrep.2025.115603
Functional characterization of the ATOH1 molecular subtype indicates a pro-metastatic role in small cell lung cancer
Abstract
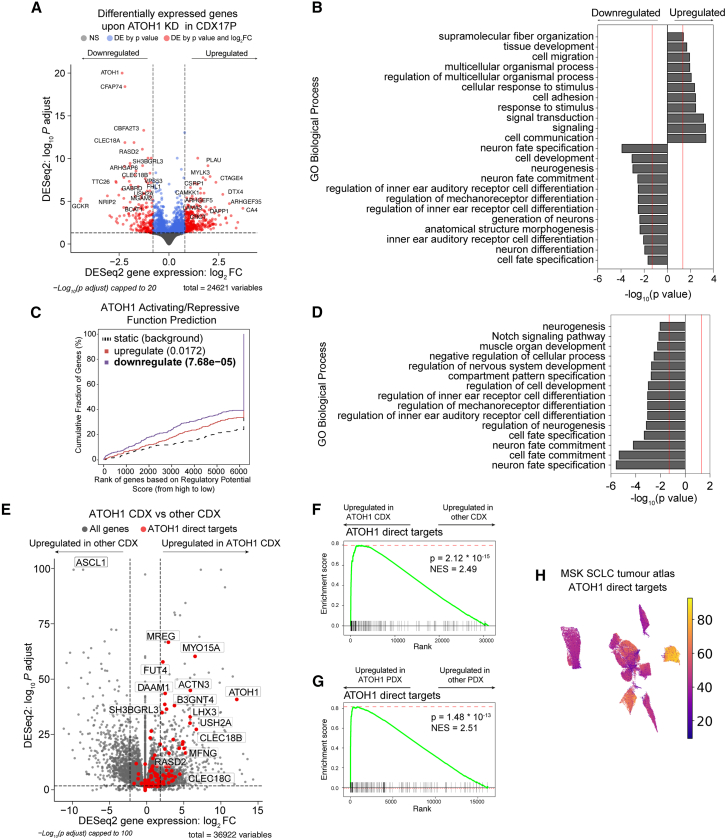
Molecular subtypes of small cell lung cancer (SCLC) have been described based on differential expression of the transcription factors (TFs) ASCL1, NEUROD1, and POU2F3 and immune-related genes. We previously reported an additional subtype based on expression of the neurogenic TF ATOH1 within our SCLC circulating tumor cell-derived explant (CDX) model biobank. Here, we show that ATOH1 protein is detected in 7 of 81 preclinical models and 16 of 102 clinical samples of SCLC. In CDX models, ATOH1 directly regulates neurogenesis and differentiation programs, consistent with roles in normal tissues. In ex vivo cultures of ATOH1+ CDXs, ATOH1 is required for cell survival. In vivo, ATOH1 depletion slows tumor growth and suppresses liver metastasis. Our data validate ATOH1 as a bona fide lineage-defining TF of SCLC with cell survival and pro-metastatic functions. Further investigation exploring ATOH1-driven vulnerabilities for targeted treatment with predictive biomarkers is warranted.
Keywords: ATOH1; CDX; CP: Cancer; CTC-derived explant models; SCLC; SCLC molecular subtype; metastasis; small cell lung cancer.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests F.B. declares advisory board honoraria, speaker fees, and research funding from Amgen. C.D. declares research funding/educational research grants from AstraZeneca, Astex Pharmaceuticals, Biomodal, Bioven, Amgen, Carrick Therapeutics, Merck AG, Taiho Oncology, GSK, Bayer, Boehringer Ingelheim, Roche, BMS, Novartis, Celgene, Epigene Therapeutics Inc, Angle PLC, Menarini, Clearbridge Biomedics, Thermo Fisher Scientific, and Neomed Therapeutics; consultancy and/or advisory board honoraria from Biocartis, Merck, AstraZeneca, GRAIL, Boehringer Ingelheim, and VHIO; and personal remuneration from IFOM. C.M.R. has consulted for Amgen, AstraZeneca, Daiichi Sankyo, Hoffman-La Roche, and Jazz; serves on the scientific advisory boards of Auron, DISCO, and Earli and received royalty payments for DLL3-directed therapeutics licensing. J.M.C. consulted for Sonata Therapeutics.
Figures






Update of
-
Functional Characterisation of the ATOH1 Molecular Subtype Indicates a Pro-Metastatic Role in Small Cell Lung Cancer.bioRxiv [Preprint]. 2024 Feb 17:2024.02.16.580247. doi: 10.1101/2024.02.16.580247. bioRxiv. 2024. Update in: Cell Rep. 2025 May 27;44(5):115603. doi: 10.1016/j.celrep.2025.115603. PMID: 38405859 Free PMC article. Updated. Preprint.
References
-
- Forman D. International Agency for Research on Cancer; 2014. Cancer Incidence in Five Continents: Volume X.
-
- American Cancer Society. Cancer Facts & Figures. 2022;2022 https://www.cancer.org
-
- Bunn P.A., Jr., Minna J.D., Augustyn A., Gazdar A.F., Ouadah Y., Krasnow M.A., Berns A., Brambilla E., Rekhtman N., Massion P.P., et al. Small Cell Lung Cancer: Can Recent Advances in Biology and Molecular Biology Be Translated into Improved Outcomes? J. Thorac. Oncol. 2016;11:453–474. doi: 10.1016/j.jtho.2016.01.012. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
