

Lisocabtagene maraleucel for R/R LBCL in patients not intended for HSCT: final results of the phase 2 PILOT study
- PMID: 40305658
- PMCID: PMC12305224
- DOI: 10.1182/bloodadvances.2024015262
Lisocabtagene maraleucel for R/R LBCL in patients not intended for HSCT: final results of the phase 2 PILOT study
Abstract
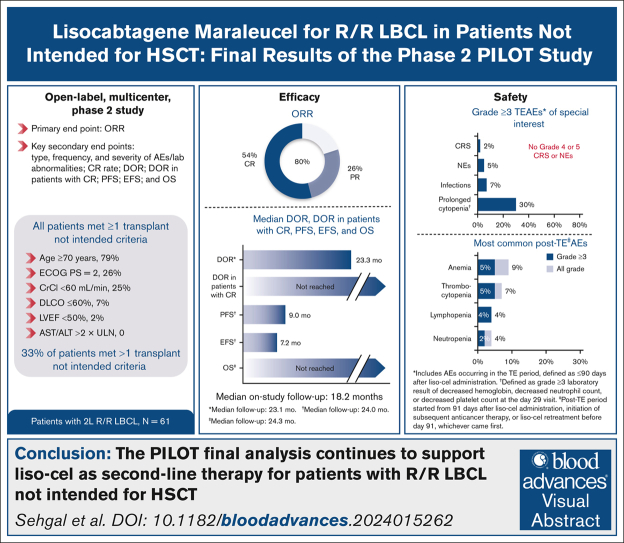
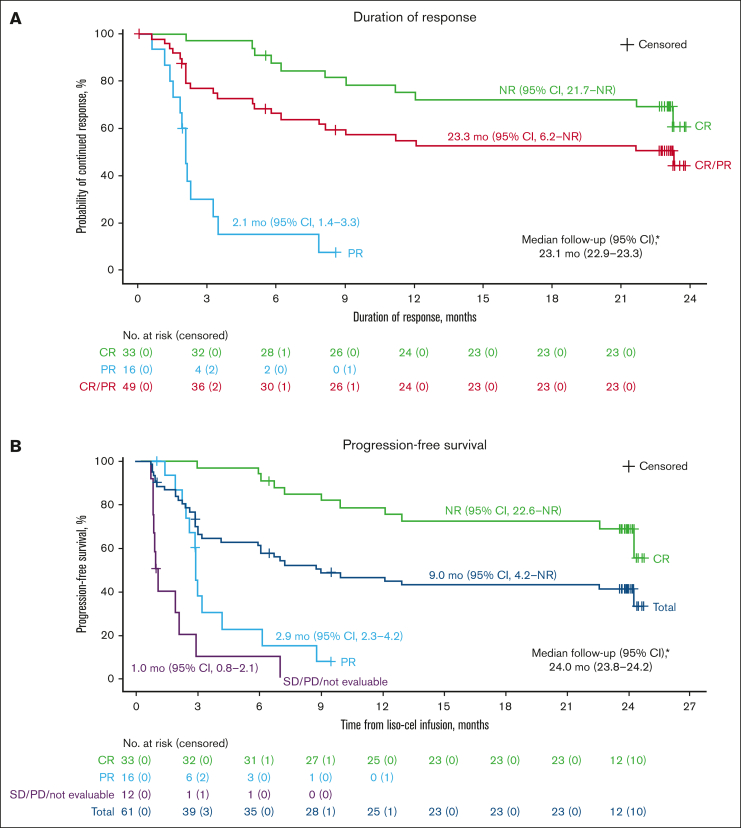
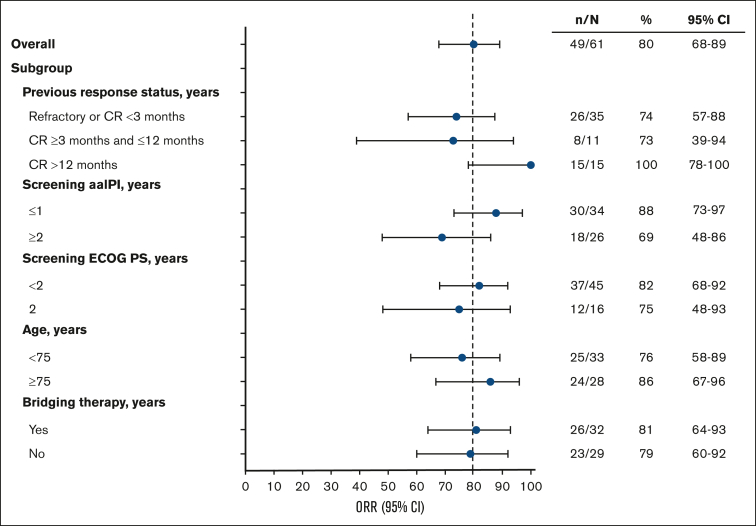
We report final analysis results from the PILOT study of lisocabtagene maraleucel (liso-cel) for patients with relapsed/refractory (R/R) large B-cell lymphoma (LBCL). Sixty-one adults with R/R LBCL who had received 1 previous line of therapy and met ≥1 hematopoietic stem cell transplantation (HSCT) not intended criterion. Overall response rate (primary end point) was 80%; 54% achieved complete response. After median on-study follow-up of 18.2 months, median duration of response was 23.3 months (95% confidence interval [CI], 6.2 to not reached [NR]). Median progression-free survival (PFS) was 9.0 months (95% CI, 4.2 to NR), median overall survival (OS) was NR (95% CI, 16.3 to NR), and 18-month PFS and OS rates were 43% (95% CI, 30-55) and 59% (95% CI, 45-70), respectively. In the treatment-emergent (TE) period (≤90 days after liso-cel administration), 79% had grade ≥3 adverse events (AEs), 38% had cytokine release syndrome (2% grade 3; no grade 4/5), 31% had neurological events (5% grade 3; no grade 4/5), and 7% had grade ≥3 infections. Of 57 patients in the post-TE period (≥91 days after liso-cel administration), 18% experienced grade ≥3 AEs; 1 patient had grade ≥3 infections. Thirty patients in the leukapheresis set (n = 74) died, mostly of disease progression (n = 24). In this population with high incidence of high-grade B-cell lymphoma, primary-refractory disease, advanced age, and comorbidities, liso-cel demonstrated durable efficacy and a favorable safety profile, consistent with previous reports. These results support liso-cel as second-line therapy for this underserved population of patients with R/R LBCL not intended for HSCT. This trial was registered at www.clinicaltrials.gov as #NCT03483103.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: A.S. declares research funding from Kite/Gilead, Juno Therapeutics, a Bristol-Myers Squibb Company, Chimagen, and CytoAgents. D.H. declares speakers bureau fees from Bristol Myers Squibb. P.A.R. declares consulting fees from AbbVie, ADC Therapeutics, Bristol Myers Squibb, BeiGene, CVS Caremark, Roche/Genentech, Genmab, Intellia Therapeutics, Janssen, Kite/Gilead, Nektar Therapeutics, Novartis, Nurix Therapeutics, Pharmacyclics, and Sana Biotechnology; speakers bureau fees from Kite Pharma; and travel support from Nektar Therapeutics. N.G. declares consultancy fees from Seagen, TG Therapeutics, AstraZeneca, Pharmacyclics, Janssen, Bristol Myers Squibb, Gilead Sciences, Kite Pharma, BeiGene, Incyte, Lava Therapeutics, Roche/Genentech, Novartis, Loxo Oncology, AbbVie, Genmab, Adaptive Biotech, and ADC Therapeutics; research funding from TG Therapeutics, Roche/Genentech, Bristol Myers Squibb, Gilead Sciences, MorphoSys, AbbVie, and Pharmacyclics; speakers bureau fees from AstraZeneca, Janssen, Pharmacyclics, Kite Pharma, Bristol Myers Squibb, and Epizyme; and membership on a board of directors or advisory committee for Roche NHL Solutions Panel. M.H. declares research support from ADC Therapeutics, Astellas Pharma, Spectrum Pharmaceuticals, and Takeda Pharmaceutical; consultancy fees from AbbVie, ADC Therapeutics, Autolus, Bristol Myers Squibb, Caribou Biosciences, CRISPR Therapeutics, Genmab, Kite Pharma, and Omeros; and speakers bureau fees from ADC Therapeutics, AstraZeneca, BeiGene, CRISPR Therapeutics, DMC Inc, Genentech, Kite Pharma, and Myeloid Therapeutics. G.C.H. declares research funding from AstraZeneca and Incyte; speakers bureau participation for Missouri Oncology Society; travel support from Ono Pharmaceutical, Genmab, and Missouri Oncology Society; advisory board participation with AstraZeneca, Daiichi Sankyo, Genmab, Janssen, Ono Pharmaceutical, Rapa Therapeutics, and Sobi; and is an equity holder of AXIM Biotechnologies, AbbVie, Aimmune Therapeutics, Biogen, bluebird Bio, Cardinal Health, CareTrust REIT, Cellectis, Charlotte’s Web Holdings, Clovis Oncology, CVS Health, GW Pharmaceuticals, Insys Therapeutics, Merck, Micron Technology, Medical Properties Trust, Moderna, Mustang Bio, NeoGenomics Laboratories, OPKO Health, Viatris, and Zevra Therapeutics. P.M.R. declares a grant from Genentech; speakers bureau participation for Kite Pharma; and advisory board membership with Caribou Biosciences and Kite Pharma. N.D.W.-J. declares research funding from Astex Pharmaceuticals, Merck, and Genentech; and advisory board participation with BeiGene. J.E. declares speakers bureau participation for Bristol Myers Squibb, Genmab, and Kite Pharma. R.N. declares research funding from AbbVie, Bristol Myers Squibb, Genentech, Kite/Gilead, MorphoSys, and Pharmacyclics; and advisory board participation with AbbVie, ADC Therapeutics, AstraZeneca, BeiGene, Genentech, Kite/Gilead, Incyte, Janssen, Lava Therapeutics, Lilly, and Novartis. R.C. declares speakers bureau participation for AbbVie. S.F. declares speakers bureau participation for AbbVie, Bristol Myers Squibb, and Genmab. V.A.C., B.Y., Z.Y., K.O., and J.T. are current employees and equity holders of Bristol Myers Squibb. L.I.G. declares consultancy fees from Ono Pharmaceutical; advisory board participation for Bristol Myers Squibb and Kite Pharma; data and safety monitoring board participation for Janssen; is a cofounder of Zylem Biosciences; and reports patents for nanoparticles for cancer therapy (PCT/US2020/051549) and nanostructures for treating cancer and other conditions (PCT/US2013/027431). The remaining authors declare no competing financial interests.
J.E.G. is retired from the Earle A. Chiles Research Institute, Portland, OR.
Figures


References
-
- Kamdar M, Solomon SR, Arnason J, et al. Lisocabtagene maraleucel versus standard of care with salvage chemotherapy followed by autologous stem cell transplantation as second-line treatment in patients with relapsed or refractory large B-cell lymphoma (TRANSFORM): results from an interim analysis of an open-label, randomised, phase 3 trial. Lancet. 2022;399(10343):2294–2308. - PubMed
-
- Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N Engl J Med. 2022;386(7):640–654. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
