

Effects of Deep Learning-Based Reconstruction on the Quality of Accelerated Contrast-Enhanced Neck MRI
- PMID: 40307199
- PMCID: PMC12055266
- DOI: 10.3348/kjr.2024.1059
Effects of Deep Learning-Based Reconstruction on the Quality of Accelerated Contrast-Enhanced Neck MRI
Abstract
Objective: To compare the quality of deep learning-reconstructed turbo spin-echo (DL-TSE) and conventionally interpolated turbo spin-echo (Conv-TSE) techniques in contrast-enhanced MRI of the neck.
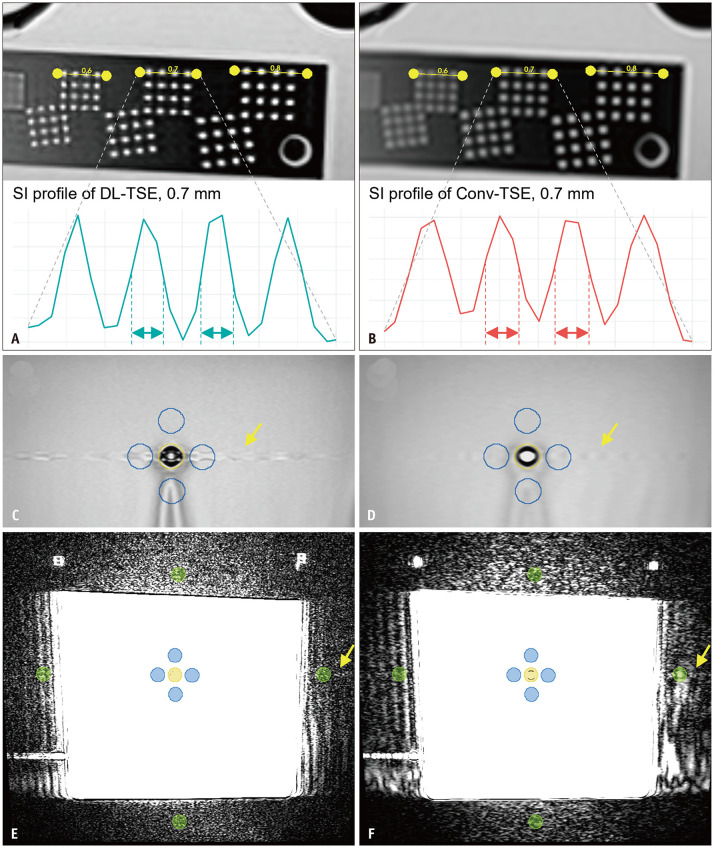
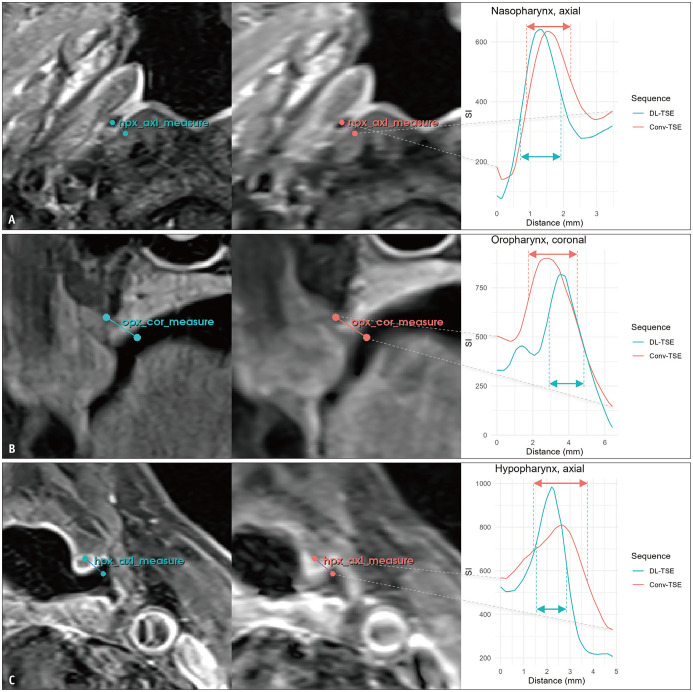
Materials and methods: Contrast-enhanced T1-weighted DL-TSE and Conv-TSE images were acquired using 3T scanners from 106 patients. DL-TSE employed a closed-source, 'work-in-progress' (WIP No. 1062, iTSE, version 10; Siemens Healthineers) algorithm for interpolation and denoising to achieve the same in-plane resolution (axial: 0.26 × 0.26 mm²; coronal: 0.29 × 0.29 mm²) while reducing scan times by 15.9% and 52.6% for axial and coronal scans, respectively. The full width at half maximum (FWHM) and percent signal ghosting were measured using stationary and flow phantom scans, respectively. In patient images, non-uniformity (NU), contrast-to-noise ratio (CNR), and regional mucosal FWHM were evaluated. Two neuroradiologists visually rated the patient images for overall quality, sharpness, regional mucosal conspicuity, artifacts, and lesions using a 5-point Likert scale.
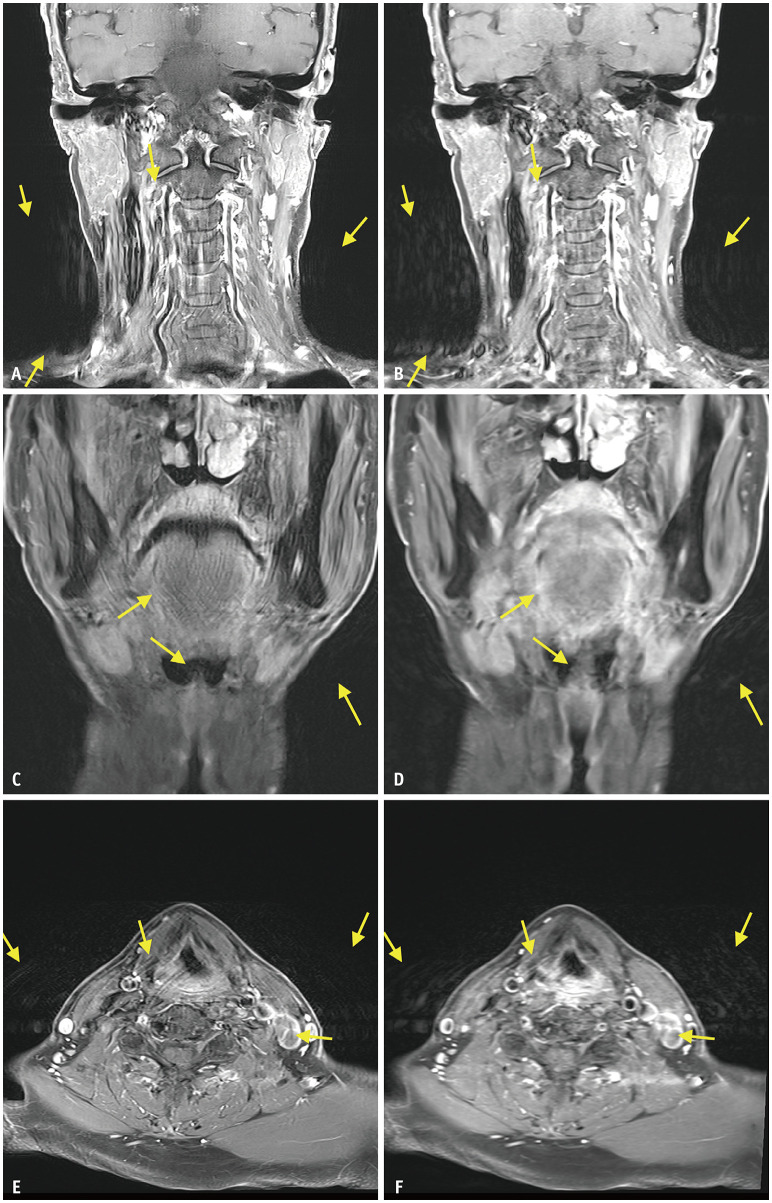
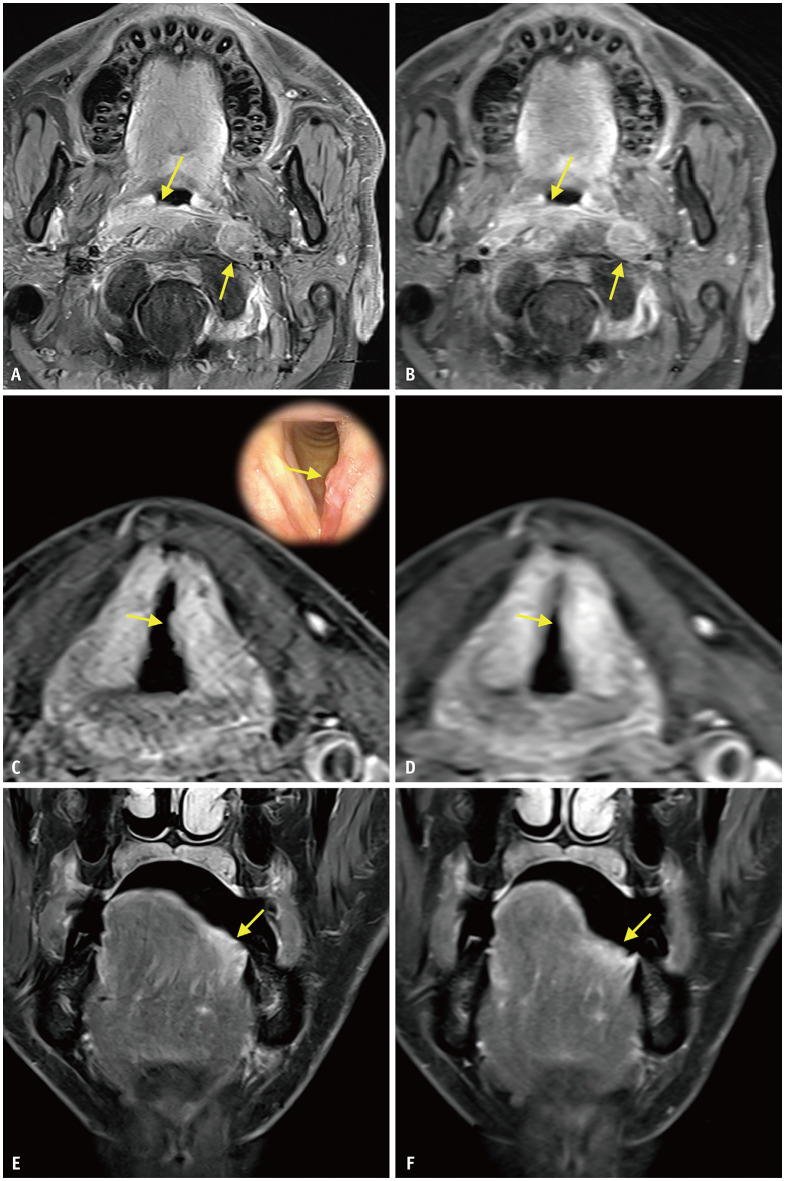
Results: FWHM in the stationary phantom scan was consistently sharper in DL-TSE. The percent signal ghosting outside the flow phantom was lower in DL-TSE (0.06% vs. 0.14%) but higher within the phantom (8.92% vs. 1.75%) compared to Conv-TSE. In patient scans, DL-TSE showed non-inferior NU and higher CNR. Regional mucosal FWHM was significantly better in DL-TSE, particularly in the oropharynx (coronal: 1.08 ± 0.31 vs. 1.52 ± 0.46 mm) and hypopharynx (coronal: 1.26 ± 0.35 vs. 1.91 ± 0.56 mm) (both P < 0.001). DL-TSE demonstrated higher overall image quality (axial: 4.61 ± 0.49 vs. 3.32 ± 0.54) and sharpness (axial: 4.40 ± 0.56 vs. 3.11 ± 0.53) (both P < 0.001). In addition, mucosal conspicuity was improved, especially in the oropharynx (axial: 4.41 ± 0.67 vs. 3.40 ± 0.69) and hypopharynx (axial: 4.45 ± 0.58 vs. 3.58 ± 0.63) (both P < 0.001). Extracorporeal ghost artifacts were reduced in DL-TSE (axial: 4.32 ± 0.60 vs. 3.90 ± 0.71, P < 0.001) but artifacts overlapping anatomical structures were slightly more pronounced (axial: 3.78 ± 0.74 vs. 3.95 ± 0.72, P < 0.001). Lesions were detected with higher confidence in DL-TSE.
Conclusion: DL-based reconstruction applied to accelerated neck MRI improves overall image quality, sharpness, mucosal conspicuity in motion-prone regions, and lesion detection confidence. Despite more pronounced ghost artifacts overlapping anatomical structures, DL-TSE enables substantial scan time reduction while enhancing diagnostic performance.
Keywords: Deep learning reconstruction; Full width at half maximum; Head and neck magnetic resonance imaging; Image quality; Image sharpness; Motion artifact.
Copyright © 2025 The Korean Society of Radiology.
Conflict of interest statement
Jinhee Jang, an Editorial Board Member of the
Figures
Comment in
-
Commentary on "Effects of Deep Learning-Based Reconstruction on the Quality of Accelerated Contrast-Enhanced Neck MRI".Korean J Radiol. 2026 Jan;27(1):76-77. doi: 10.3348/kjr.2025.1307. Korean J Radiol. 2026. PMID: 41494679 Free PMC article. No abstract available.
References
-
- Junn JC, Soderlund KA, Glastonbury CM. Imaging of head and neck cancer with CT, MRI, and US. Semin Nucl Med. 2021;51:3–12. - PubMed
-
- Avey G. Technical improvements in head and neck MR imaging: at the cutting edge. Neuroimaging Clin N Am. 2020;30:295–309. - PubMed
-
- Sartoretti E, Sartoretti-Schefer S, van Smoorenburg L, Binkert CA, Schwenk Á, Gutzeit A, et al. Contrast-enhanced T1-weighted head and neck MRI: prospective intraindividual image quality comparison of spiral GRE, cartesian GRE, and cartesian TSE sequences. AJR Am J Roentgenol. 2022;218:132–139. - PubMed
-
- Seo M, Yoon J, Choi Y, Nickel D, Jang J, Shin NY, et al. Image quality of high-resolution 3-dimensional neck MRI using CAIPIRINHA-VIBE and GRASP-VIBE: an intraindividual comparative study. Invest Radiol. 2022;57:711–719. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
