

Global burden of female infertility attributable to sexually transmitted infections and maternal sepsis: 1990-2021 and projections to 2050
- PMID: 40307311
- PMCID: PMC12043824
- DOI: 10.1038/s41598-025-94259-9
Global burden of female infertility attributable to sexually transmitted infections and maternal sepsis: 1990-2021 and projections to 2050
Abstract
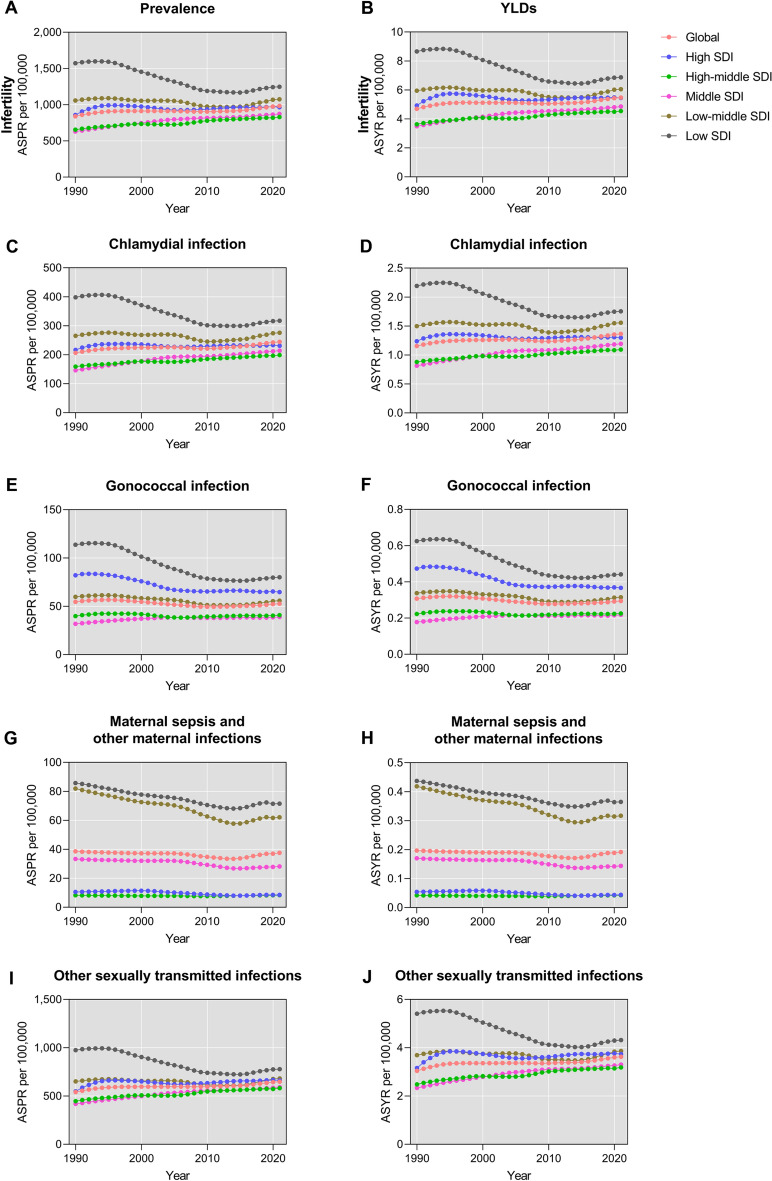
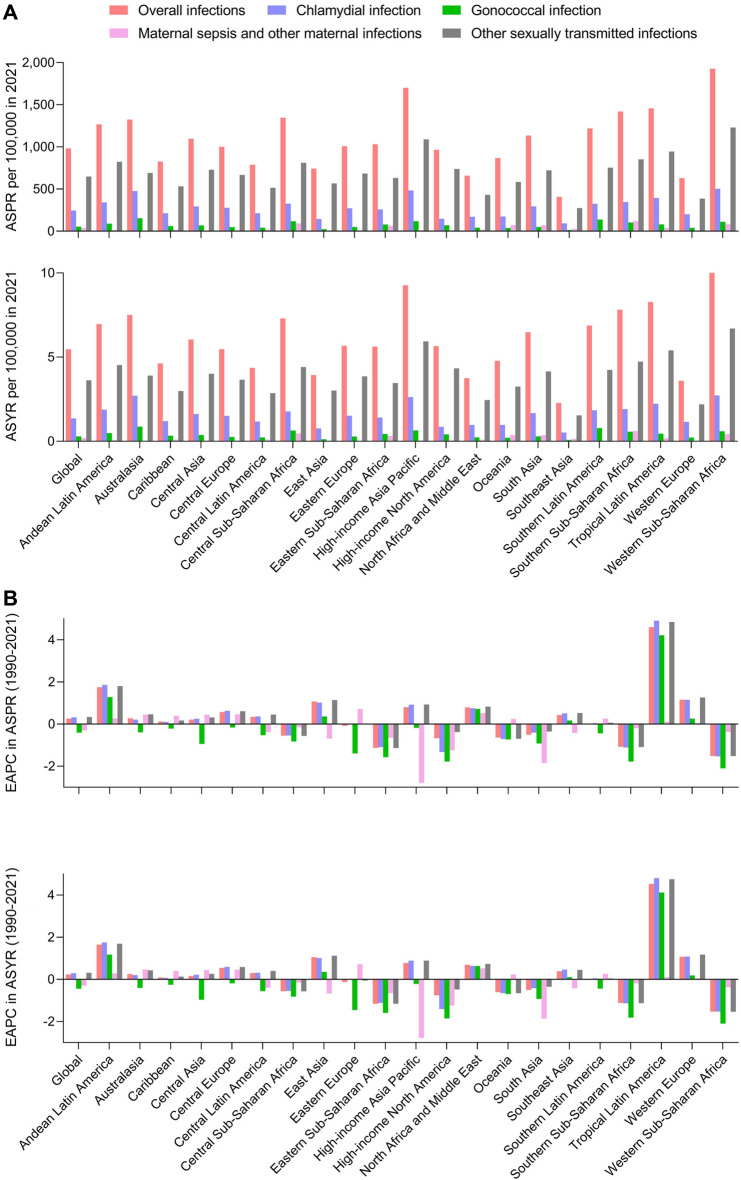
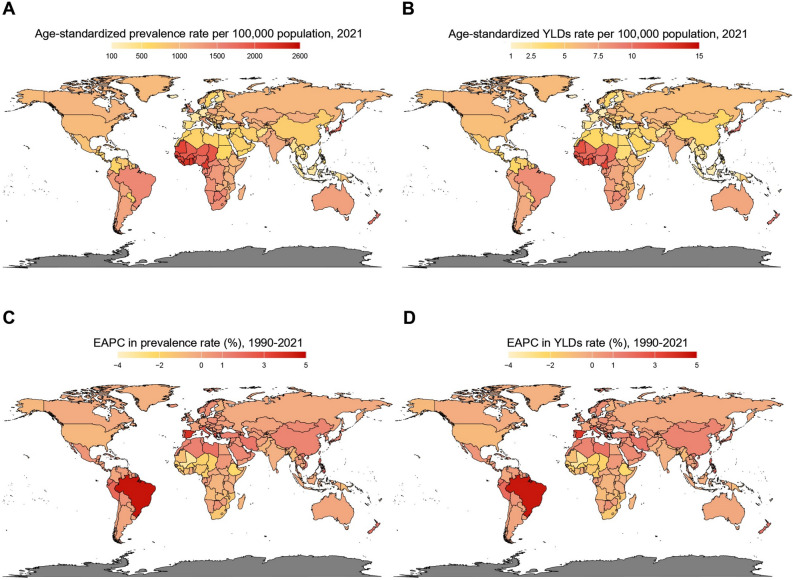
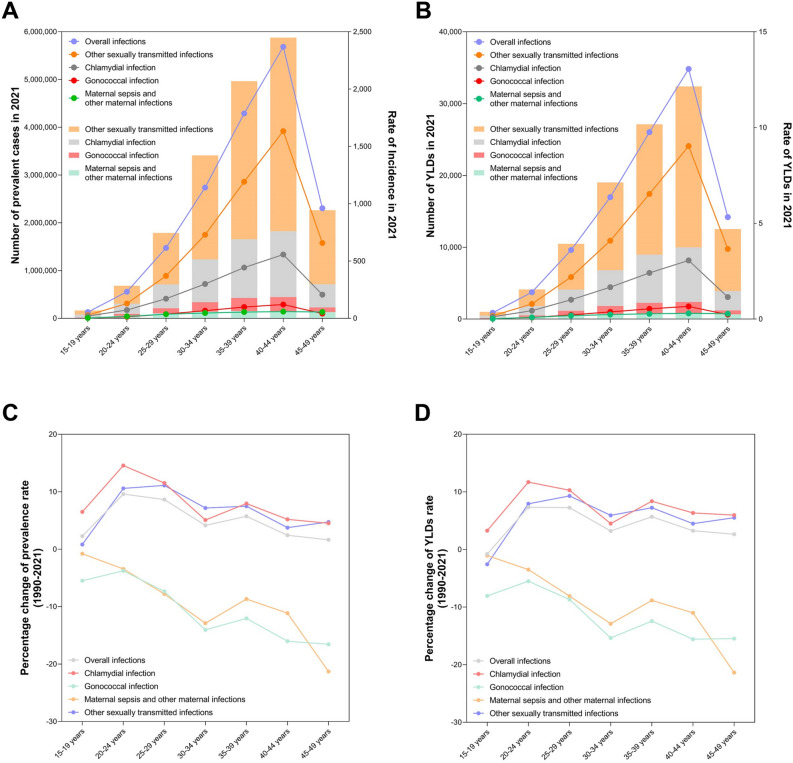
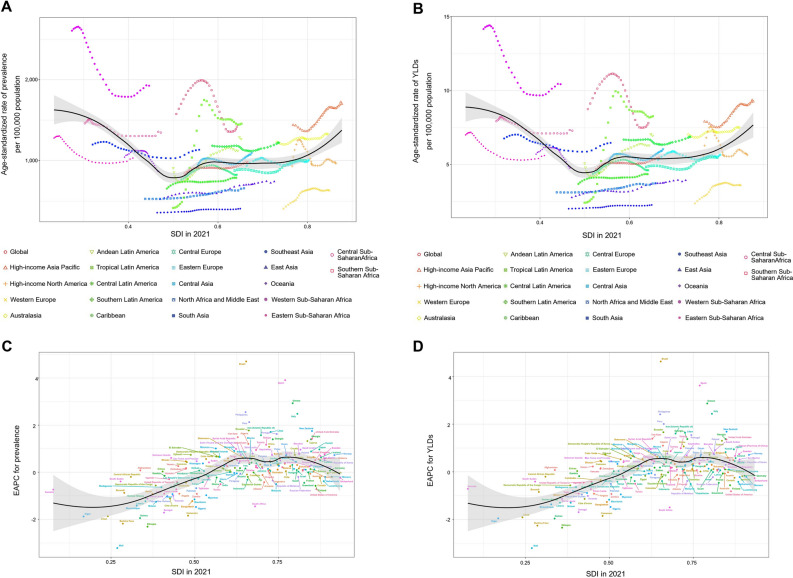
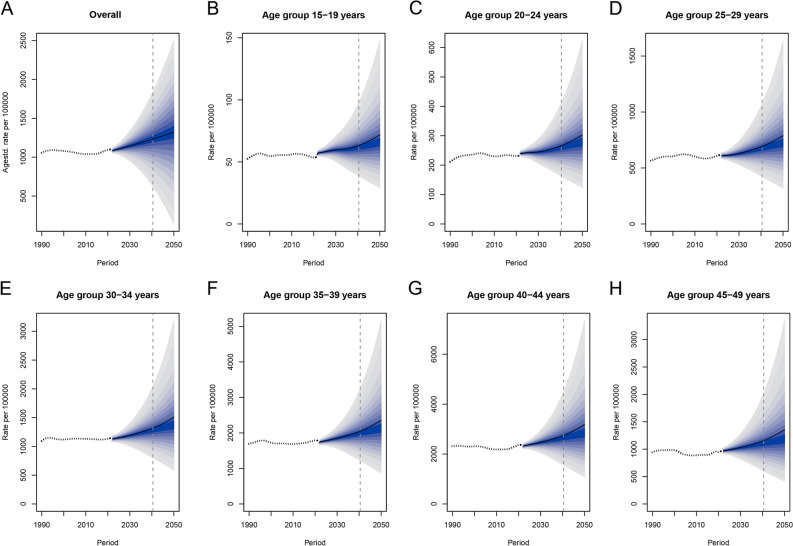
Infectious diseases, such as sexually transmitted infections (STIs) and maternal sepsis, are major contributors to female infertility, creating a substantial burden on women of reproductive age. Based on Global Burden of Disease (GBD) 2021, this study analyzed the global trends and regional disparities in infection-related infertility for women aged 15-49 and projected future burdens. Our result showed that from 1990 to 2021, global age-standardized prevalence rate (ASPR) rose from 839.52 to 982.37 per 100,000 with estimated annual percentage change (EAPC) (0.26 [0.19 to 0.33]), and years lived with disability (YLDs) increasing from 62.81 to 106.69 thousand (EAPC 0.23 [0.16 to 0.31]), and was predicted to continue rising from 2022 to 2050. The disease burden showed significant regional disparities, low socio-demographic index (SDI) regions had the highest ASPR (1247.25 per 100,000 [1085.17 to 1443.57]) but also the fastest decline (EAPC -1.17 [-1.34 to -0.99]), and Western Sub-Saharan Africa (ASPR 1,925.52 [1655.35 to 2241.71] per 100,000) are the regions with highest burden. The disease burden increased with age, peaking at 40-44 years, and was inversely associated with SDI. These findings provide essential insights for policymakers to develop targeted strategies to prevent and control infection-related infertility, particularly in low-SDI regions.
Keywords: Global burden of disease; Infections; Infertility; Maternal sepsis; Prevalence; Sexually transmitted infections.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
