

Extracellular vesicle digital scoring assay for assessment of treatment responses in hepatocellular carcinoma patients
- PMID: 40307890
- PMCID: PMC12044846
- DOI: 10.1186/s13046-025-03379-7
Extracellular vesicle digital scoring assay for assessment of treatment responses in hepatocellular carcinoma patients
Abstract
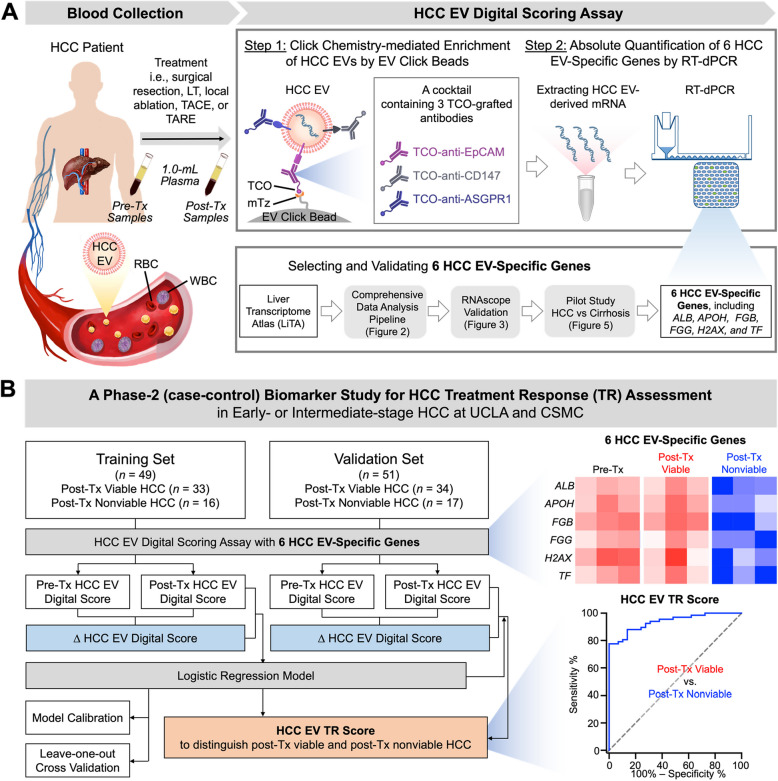
Background: There are no validated biomarkers for assessing hepatocellular carcinoma (HCC) treatment response (TR). Extracellular vesicles (EVs) are promising circulating biomarkers that may detect minimal residual disease in patients with treated HCC.
Methods: We developed the HCC EV TR Score using HCC EV Digital Scoring Assay involving click chemistry-mediated enrichment of HCC EVs, followed by absolute quantification of HCC EV-specific genes by RT-digital PCR. Six HCC EV-specific genes were selected and validated through i) a comprehensive data analysis pipeline with an unprecedentedly large collection of liver transcriptome datasets (n = 9,160), ii) RNAscope validation on HCC tissues (n = 6), and iii) a pilot study on early- or intermediate-stage HCC and liver cirrhosis patients (n = 70). The performance of HCC EV TR Score was assessed in a phase-2 retrospective case-control study (n = 100).
Results: HCC EV TR Scores, calculated from pre- and post-treatment plasma samples in the phase-2 case-control study, accurately differentiated post-treatment viable from nonviable HCC in the training (area under the ROC curve [AUROC] of 0.90, n = 49) and validation set (AUROC of 0.88, n = 51). At an optimal cutoff of 0.76 identified in the training set, HCC EV TR Score had high accuracy in detecting viable tumors (sensitivity: 76.5%, specificity: 88.2%) and found residual disease not initially observed on MRI in six patients with a median lead time of 63 days.
Conclusions: This EV-based digital scoring approach shows great promise to augment cross-sectional imaging for the assessment of HCC treatment response.
Keywords: Extracellular Vesicle; Hepatocellular Carcinoma; Liquid Biopsy; Treatment Responses.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Office of the Human Research Protection Program at University of California, Los Angeles (#14–000197, #10–000236-AM- 00021 and #20–001197) and the Office of Research Compliance and Quality Improvement at Cedars-Sinai Medical Center (#00000066, #00042197, and #00033050). Samples were collected only after obtaining written informed consent from the participants. Consent for publication: Not applicable. The manuscript does not contain any individual personal data. Competing interests: Dr. Ju Dong Yang provides a consulting service for FujiFilm Medical Sciences, Exact Sciences, AstraZeneca, Eisai, Exelixis, and Merck. Dr. Yazhen Zhu is a co-founder and shareholder in Eximius Diagnostics Corp.. Dr. Hsian-Rong Tseng would like to disclose that he has financial interests in CytoLumina Technologies Corp., Pulsar Therapeutics Corp., and. Eximius Diagnostics Corp. Dr. Vatche Agopian provides a consulting service for Merck, Eximius Diagnostics Corp, and Early Diagnostics Corp. Dr. Amit Singal has served as a consultant or on advisory boards for Genentech, AztraZeneca, Eisai, Exelixis, Bayer, Elevar, Boston Scientific, Sirtex, Histosonics, FujiFilm Medical Sciences, Exact Sciences, Roche, Abbott, Glycotest, Freenome, and GRAIL.
Figures







References
MeSH terms
Substances
Grants and funding
- U01 CA230705/CA/NCI NIH HHS/United States
- K08 CA259534/CA/NCI NIH HHS/United States
- R21 CA280444/CA/NCI NIH HHS/United States
- R01 CA255727/CA/NCI NIH HHS/United States
- R01CA277530, R01CA255727, R01CA253651, R01CA253651-04S1, R21CA280444, R01CA246304, U01EB026421, K08CA259534, R44CA288163, U01CA271887, and U01CA230705/CA/NCI NIH HHS/United States
