

Analysis of Factors Relevant to the Severity of Symptoms in Children and Adolescents with Postural Orthostatic Tachycardia Syndrome
- PMID: 40310095
- PMCID: PMC12026312
- DOI: 10.3390/children12040474
Analysis of Factors Relevant to the Severity of Symptoms in Children and Adolescents with Postural Orthostatic Tachycardia Syndrome
Abstract
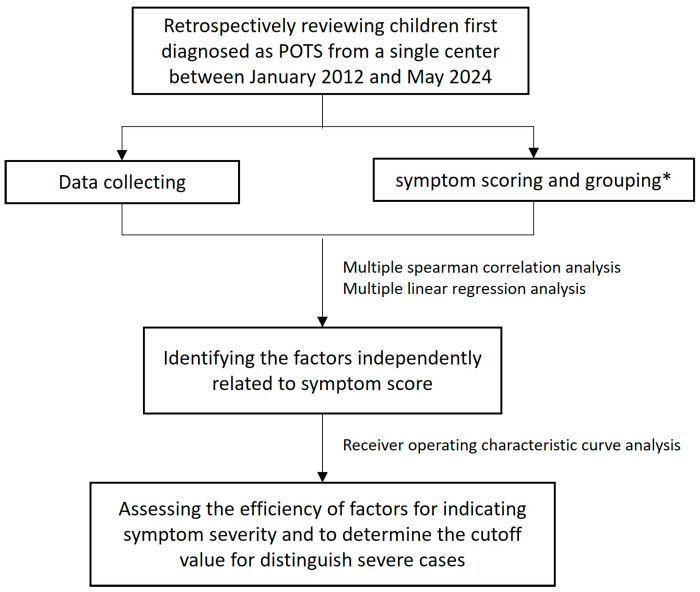
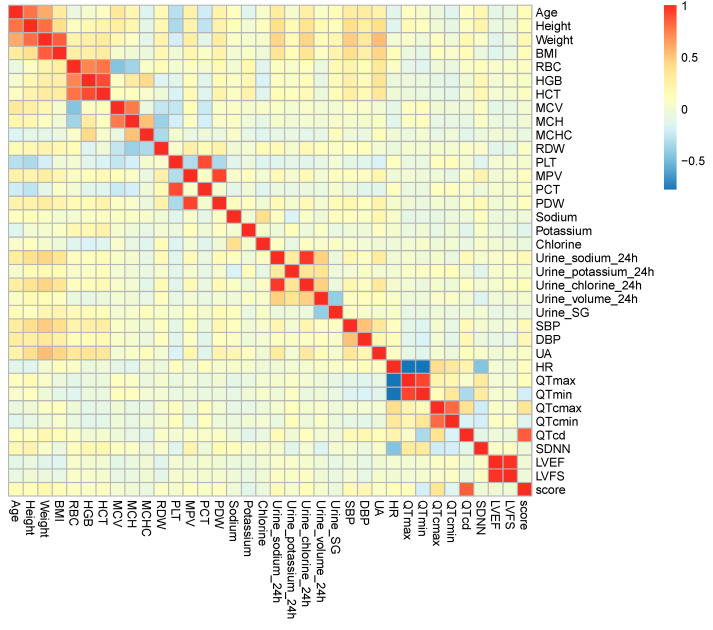
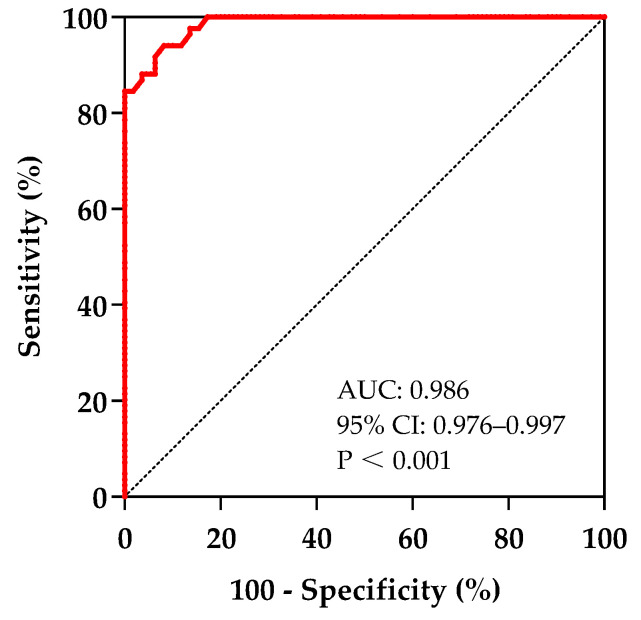
Objectives: The current study aims to investigate the factors associated with the severity of conditions for pediatric cases with postural orthostatic tachycardia syndrome (POTS). Methods: Patients hospitalized and first diagnosed with POTS were retrospectively included and reviewed. The severity of symptoms was evaluated by symptom scores (SSs). Multiple Spearman correlation analyses and multiple linear regression analyses were used to determine factors independently associated with SS. Patients were divided into the mild (SS ≤ P25) and severe (SS ≥ P75) groups to test the distinguishing efficiency of the candidate factors. The efficiency of each independently correlated factor in indicating the condition of children with POTS was assessed by the receiver operating characteristic (ROC) curve. Results: A series of 296 pediatric patients aged 5-17 years suffering from POTS were included. Multiple Spearman correlation analyses and multiple linear regression analyses showed that corrected QT interval dispersion (QTcd) was independently correlated with SS (p < 0.05). QTcd can be used to suggest the severity of POTS symptoms, and the area under the curve (AUC) was 0.986 (95% CI 0.976-0.997). At a threshold of QTcd = 45 ms, the sensitivity and specificity were, respectively, 94.0% and 91.8% for symptom severity indication. Conclusions: In pediatric cases with POTS, QTcd was positively correlated with their symptom severity and exhibited a strong indicative value. A QTcd of 45 ms was a valid cut-off value for indicating symptom severity.
Keywords: children; corrected QT interval dispersion; postural orthostatic tachycardia syndrome; relevant factor; symptom score; symptom severity.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Baseline Corrected QT Interval Dispersion Is Useful to Predict Effectiveness of Metoprolol on Pediatric Postural Tachycardia Syndrome.Front Cardiovasc Med. 2022 Jan 20;8:808512. doi: 10.3389/fcvm.2021.808512. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35127870 Free PMC article.
-
Acceleration index predicts efficacy of orthostatic training on postural orthostatic tachycardia syndrome in children.Eur J Pediatr. 2024 Sep;183(9):4029-4039. doi: 10.1007/s00431-024-05664-7. Epub 2024 Jul 2. Eur J Pediatr. 2024. PMID: 38955847
-
Electrocardiography-Derived Predictors for Therapeutic Response to Treatment in Children with Postural Tachycardia Syndrome.J Pediatr. 2016 Sep;176:128-33. doi: 10.1016/j.jpeds.2016.05.030. Epub 2016 Jun 16. J Pediatr. 2016. PMID: 27318378
-
Update of Individualized Treatment Strategies for Postural Orthostatic Tachycardia Syndrome in Children.Front Neurol. 2020 Jun 11;11:525. doi: 10.3389/fneur.2020.00525. eCollection 2020. Front Neurol. 2020. PMID: 32655482 Free PMC article. Review.
-
Pain Management In Pediatric Patients With Postural Orthostatic Tachycardia Syndrome: Current Insights.J Pain Res. 2019 Oct 31;12:2969-2980. doi: 10.2147/JPR.S194391. eCollection 2019. J Pain Res. 2019. PMID: 31802934 Free PMC article. Review.
References
-
- Vernino S., Bourne K.M., Stiles L.E., Grubb B.P., Fedorowski A., Stewart J.M., Arnold A.C., Pace L.A., Axelsson J., Boris J.R., et al. Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting-Part 1. Auton. Neurosci. 2021;235:102828. doi: 10.1016/j.autneu.2021.102828. - DOI - PMC - PubMed
-
- Shen W.K., Sheldon R.S., Benditt D.G., Cohen M.I., Forman D.E., Goldberger Z.D., Grubb B.P., Hamdan M.H., Krahn A.D., Link M.S., et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2017;14:e155–e217. doi: 10.1016/j.hrthm.2017.03.004. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
