

A National Trauma-Informed Adverse Childhood Experience Screening and Intervention Evaluation Project
- PMID: 40310097
- PMCID: PMC12025958
- DOI: 10.3390/children12040453
A National Trauma-Informed Adverse Childhood Experience Screening and Intervention Evaluation Project
Abstract
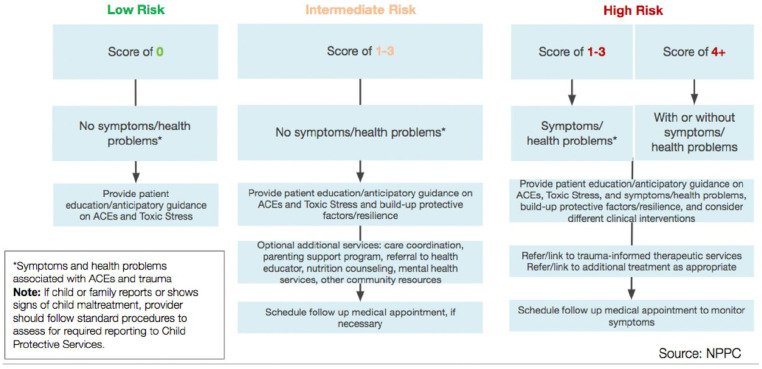
Background/objectives: Adverse childhood experiences (ACEs) are traumatic childhood events that can disrupt neurologic, endocrine, and immune regulation and increase the risk for poor health outcomes. This Trauma-Informed ACE Screening and Intervention Evaluation (TASIE) Quality Improvement (QI) Project, ECHO, evaluated (1) pediatric provider knowledge of ACEs, toxic stress, and trauma-informed care principles, (2) implementation of ACE screening and clinical response in practice, and (3) patient and provider perspectives around benefits and challenges of ACE screening.
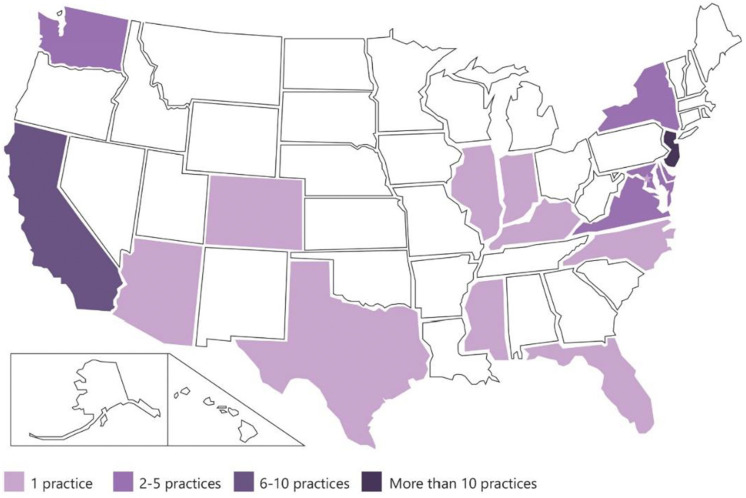
Methods: From November 2021 to May 2024, three cohorts, totaling 46 pediatric practices across the U.S., participated in the TASIE Project, which included 2 h ACE training, eight monthly 75 min ECHO sessions, and monthly QI coaching. A mixed-methods approach was used to evaluate monthly data, while patient and provider surveys and provider focus groups were used to evaluate the program.
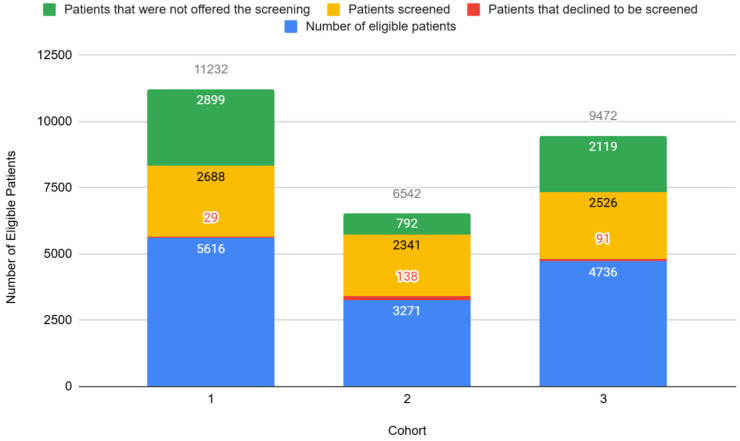
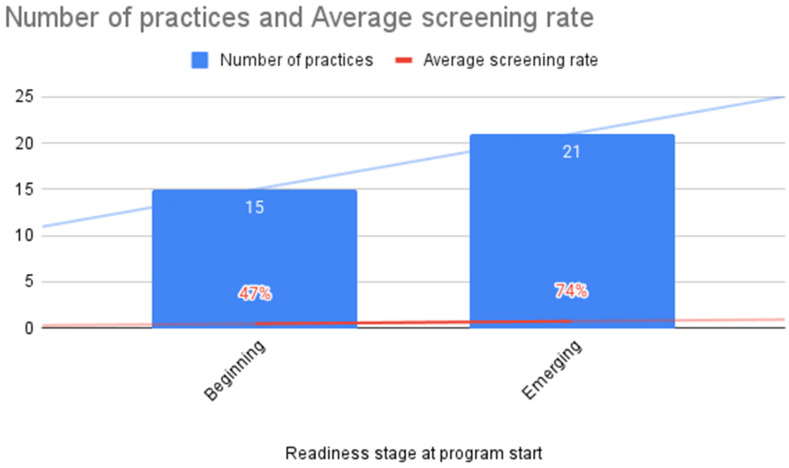
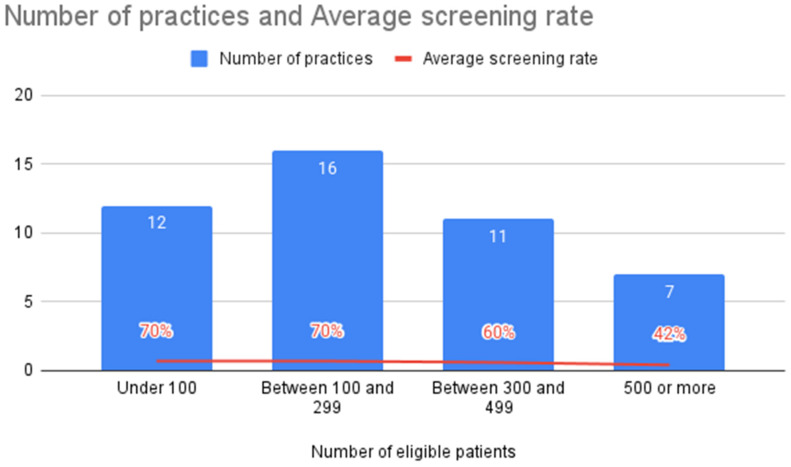
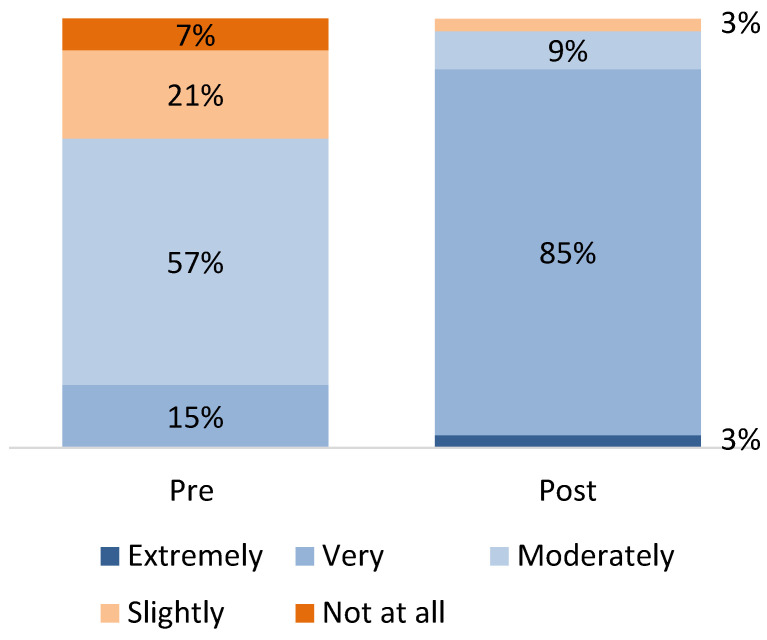
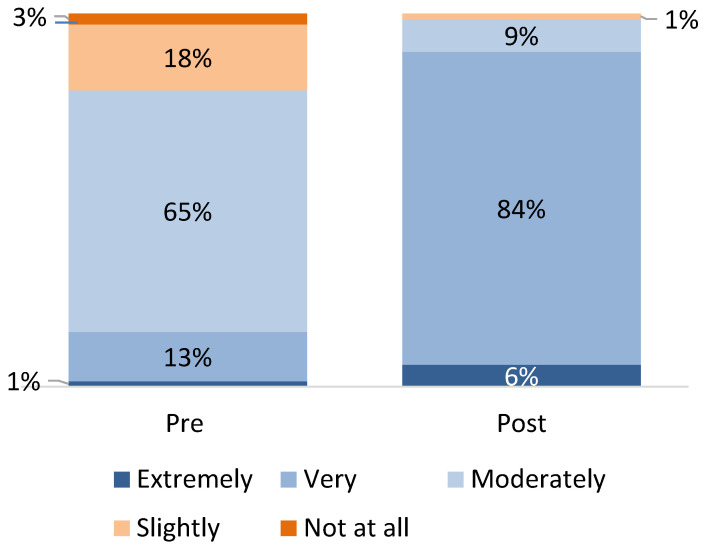
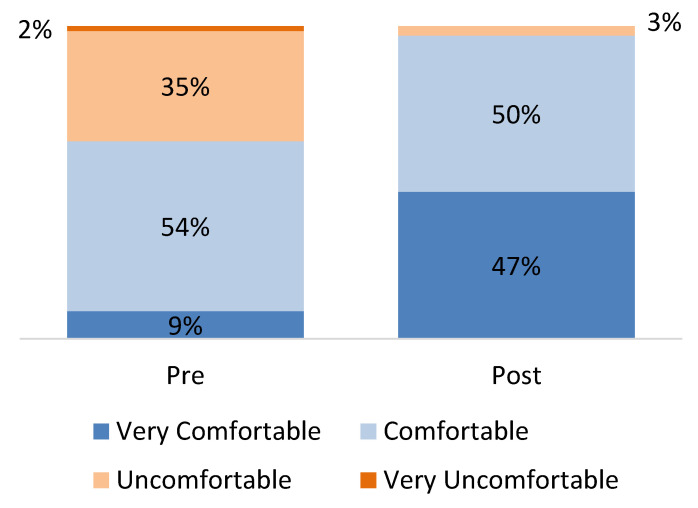
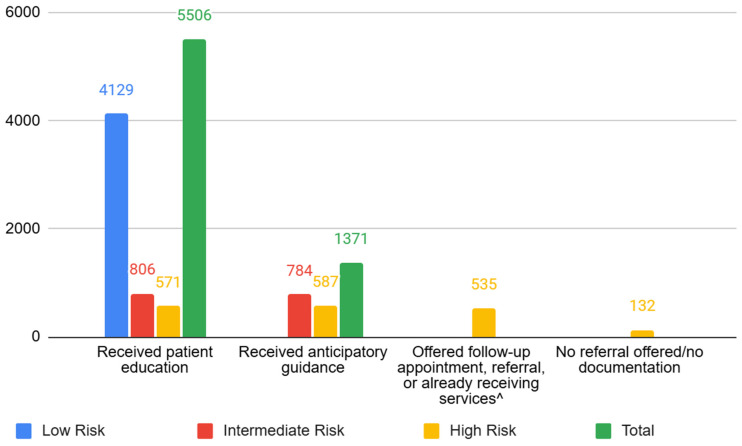
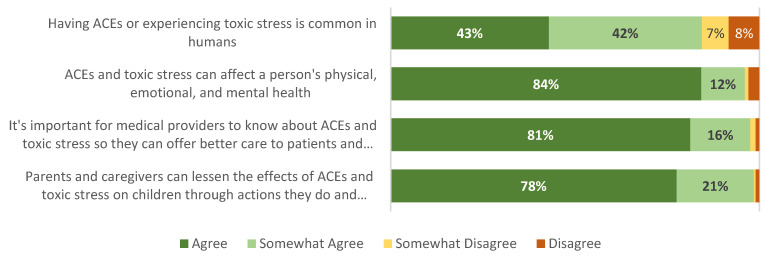
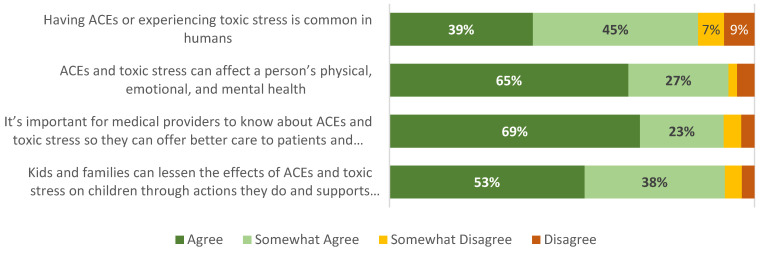
Results: All 46 participating practices implemented ACE screening by the project's conclusion. Of the patients eligible for ACE screening, over half were screened for ACEs during the program. Providers increased comfort with discussing ACEs and screening questions. During the first month, the practices were reported to have provided education to 56% of patients, and by the end of the project, this rate increased to 79% of patients. Overall, 97% of caregivers and 92% of adolescents screened agreed or somewhat agreed that it is important for providers to know about ACEs and toxic stress so they can offer better care. By the end of the project, for each cohort, providers reported that they were able to screen effectively and efficiently in routine practice and were more familiar with local resources.
Keywords: adolescent; adverse childhood experiences; caregiver; intervention; pediatric provider; practice; resilience; screening; toxic stress; trauma-informed care; wellness.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Patient-Provider Trust as a Key Component of Prenatal Screening for Adverse Childhood Experiences (ACES): A Concept Analysis.J Midwifery Womens Health. 2025 Jan-Feb;70(1):88-95. doi: 10.1111/jmwh.13660. Epub 2024 Jun 30. J Midwifery Womens Health. 2025. PMID: 38946242 Free PMC article. Review.
-
Addressing Adverse Childhood Experiences in Clinics Serving California Farmworker Communities: NACES Pilot Project Evaluation.Rand Health Q. 2024 Dec 10;12(1):1. eCollection 2024 Dec. Rand Health Q. 2024. PMID: 39664981 Free PMC article.
-
ACE-Informed Responses in Central Texas: Findings from a Needs Assessment.Soc Work Public Health. 2021 Nov 17;36(7-8):820-831. doi: 10.1080/19371918.2021.1958118. Epub 2021 Aug 12. Soc Work Public Health. 2021. PMID: 34380381
-
Screening for Adverse Childhood Experiences in Primary Care: A Quality Improvement Project.J Pediatr Health Care. 2020 Mar-Apr;34(2):122-127. doi: 10.1016/j.pedhc.2019.09.001. Epub 2019 Nov 6. J Pediatr Health Care. 2020. PMID: 31704177
-
Trauma-Informed Care in Pediatrics: A Developmental Perspective in Twelve Cases with Narratives.Perm J. 2020;24:19.045. doi: 10.7812/TPP/19.045. Epub 2019 Dec 6. Perm J. 2020. PMID: 31852045 Free PMC article. Review.
References
-
- Caserta M.T., O’Connor T.G., Wyman P.A., Wang H., Moynihan J., Cross W., Tu X., Jin X. The associations between psychosocial stress and the frequency of illness, and innate and adaptive immune function in children. Brain Behav. Immun. 2008;22:933–940. doi: 10.1016/j.bbi.2008.01.007. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
