

Washout on Contrast-Enhanced Ultrasound of Benign Focal Liver Lesions-A Review on Its Frequency and Possible Causes
- PMID: 40310346
- PMCID: PMC12025567
- DOI: 10.3390/diagnostics15080998
Washout on Contrast-Enhanced Ultrasound of Benign Focal Liver Lesions-A Review on Its Frequency and Possible Causes
Abstract
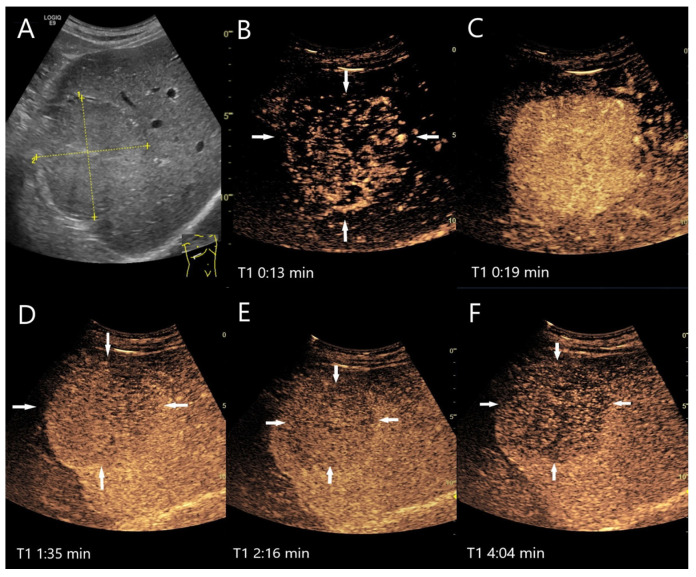
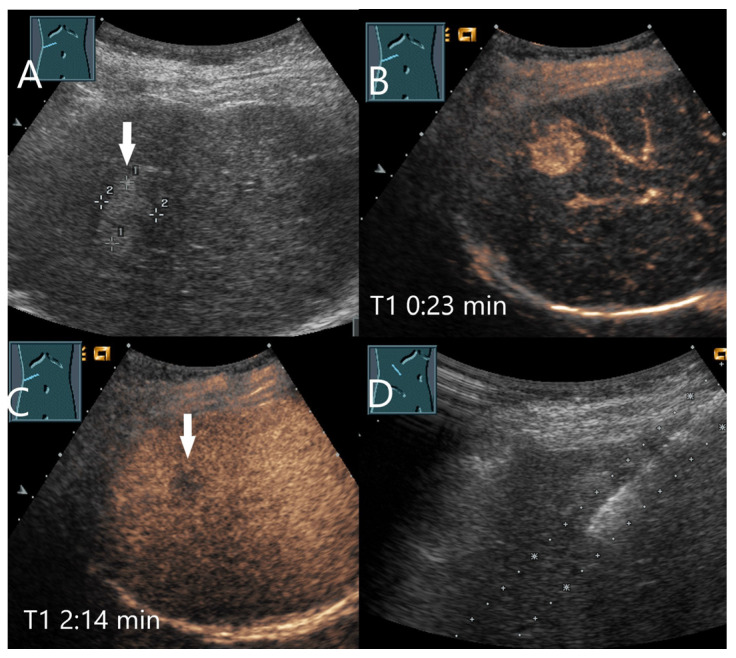
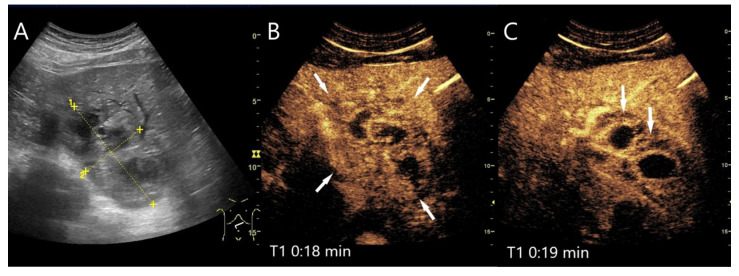
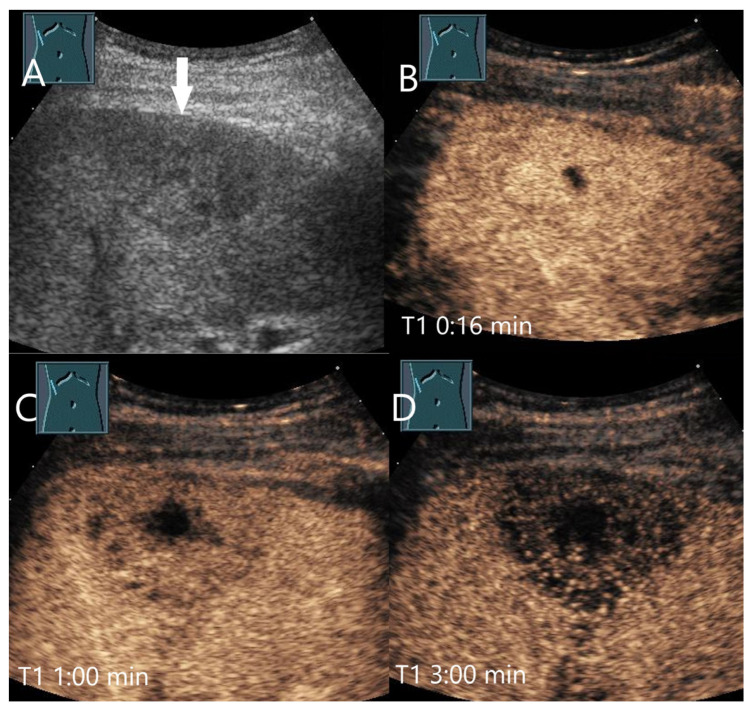
In all imaging methods, including contrast-enhanced ultrasound (CEUS), enhancement in the late phase (LP) is an important criterion for differentiating between benign and malignant focal liver lesions (FLLs). In general, malignant liver lesions are characterized by hypoenhancement and washout in the LP. A lesion with LP hyperenhancement or isoenhancement in the non-cirrhotic liver is usually benign. However, LP hypoenhancement in benign lesions is not so rare, and is even normal and the standard for some lesions, and there are exceptions for each tumor entity that can represent a diagnostic challenge. Knowing these contrast patterns and exceptions is key for correct diagnosis and patient management. The following narrative review describes the contrast behaviors and the frequency of washout and LP hypoenhancement for common as well as rare benign liver lesions and analyzes its causes.
Keywords: benign liver lesions; contrast-enhanced ultrasound (CEUS); hypoenhancement; late phase (LP); washout.
Conflict of interest statement
The authors declare that they have no financial conflicts of interest with regard to the content of this report. Martin Krix is an employee of Bracco.
Figures

References
-
- Dietrich C.F., Nolsøe C.P., Barr R.G., Berzigotti A., Burns P.N., Cantisani V., Chammas M.C., Chaubal N., Choi B.I., Clevert D.-A., et al. Guidelines and Good Clinical Practice Recommendations for Contrast-Enhanced Ultrasound (CEUS) in the Liver–Update 2020 WFUMB in Cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultrasound Med. Biol. 2020;46:2579–2604. doi: 10.1016/j.ultrasmedbio.2020.04.030. - DOI - PubMed
-
- Lee J.Y., Minami Y., Choi B.I., Lee W.J., Chou Y.-H., Jeong W.K., Park M.-S., Kudo N., Lee M.W., Kamata K., et al. The AFSUMB Consensus Statements and Recommendations for the Clinical Practice of Contrast-Enhanced Ultrasound using Sonazoid. Ultrasonography. 2020;39:191–220. doi: 10.14366/usg.20057. - DOI - PMC - PubMed
-
- Kong W., Wang W., Huang B., Ding H., Mao F. Value of wash-in and wash-out time in the diagnosis between hepatocellular carcinoma and other hepatic nodules with similar vascular pattern on contrast-enhanced ultrasound. J. Gastroenterol. Hepatol. 2014;29:576–580. doi: 10.1111/jgh.12394. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
