

Subtypes of tic disorders in children and adolescents: based on clinical characteristics
- PMID: 40312306
- PMCID: PMC12046735
- DOI: 10.1186/s12887-025-05698-2
Subtypes of tic disorders in children and adolescents: based on clinical characteristics
Abstract
Background: Tic disorder (TD) is a diverse neurodevelopmental disorder with various symptoms and comorbidities. Traditional classifications based on age onset and duration fail to adequately characterize the full clinical features of TD. This study aims to redefine TD subtypes by a comprehensive analysis of clinical features and comorbidities.
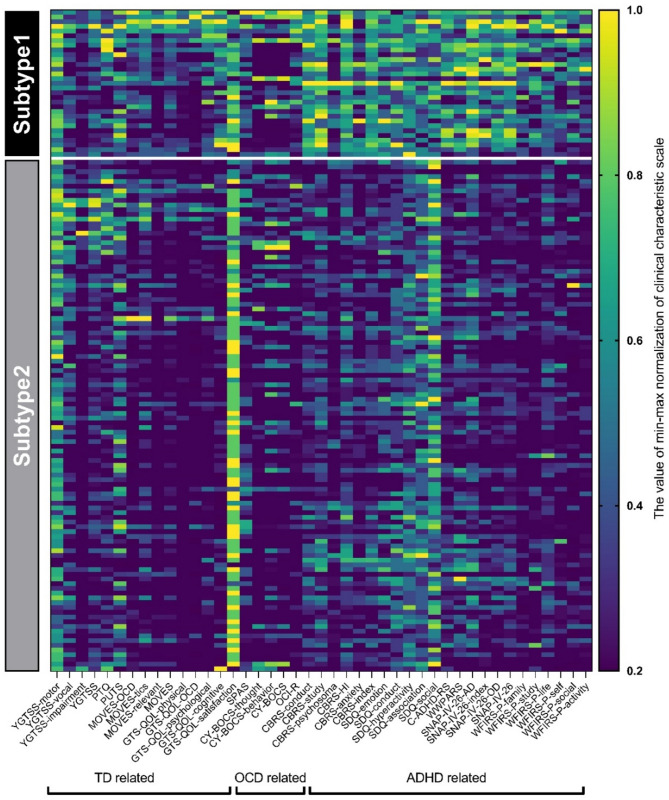
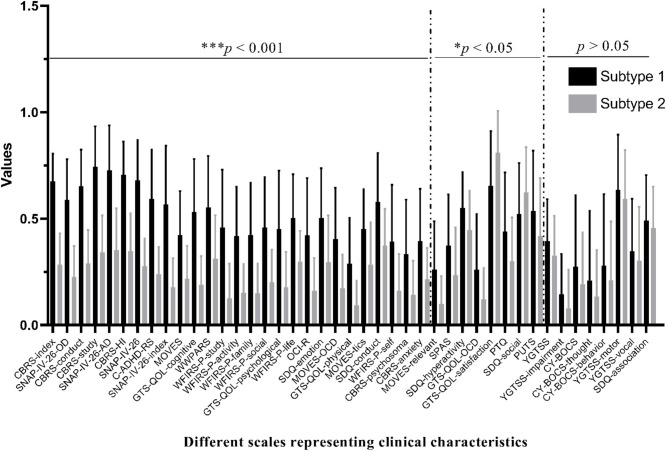
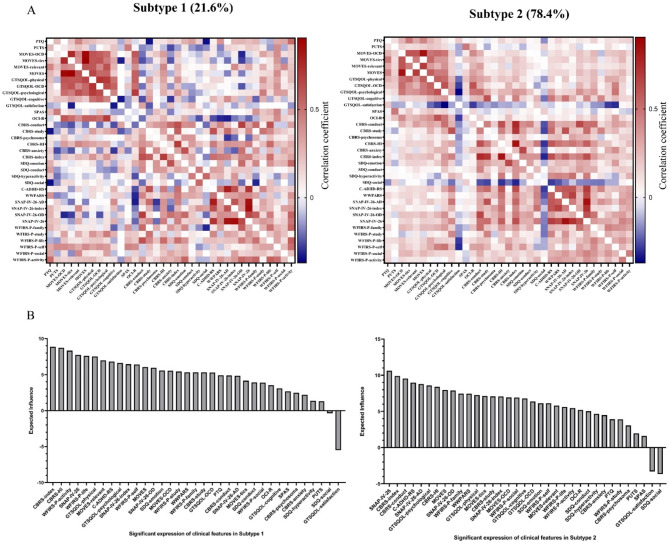
Methods: We assessed 139 children and adolescents aged 6-18 years using 14 scales covering 43 dimensions. The k-means clustering algorithm was used to identify distinct TD subtypes. Differences between these subtypes were analyzed using t-tests and network analysis, with high expected influence (EI) metric representing key symptoms within each subtype.
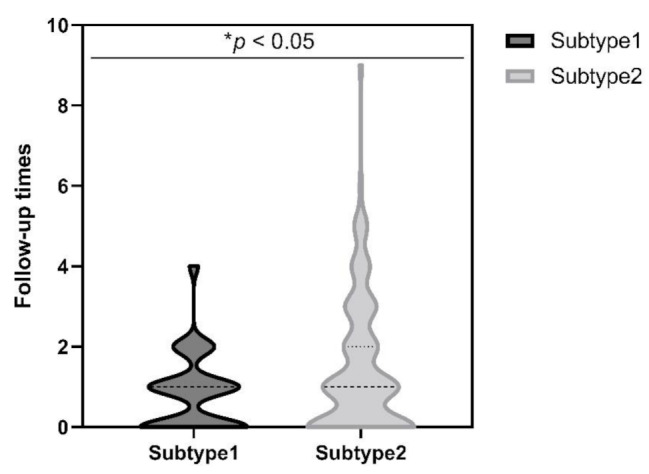
Results: We identified two distinct subtypes of TD, with 21.6% of participants classified as subtype1 and 78.4% as subtype2. Subtype1 exhibited more severe symptoms across TD, obsessive-compulsive spectrum disorders, and attention deficit hyperactivity disorder assessments compared to subtype2, with significant differences observed in 81.4% of the scale features. Network analysis revealed differences in core symptoms between the two subtypes; subtype1 primarily involved hyperactivity and vital activities, whereas subtype2 primarily involved attention deficit, hyperactivity and conduct. Furthermore, comparisons with DSM-5 classifications revealed distinct patterns, indicating the novel nature of the identified subtypes.
Conclusion: Our study identified two novel TD subtypes, highlighting its heterogeneity. Subtype 1 had more severe attention deficits and impulsivity, requiring comprehensive treatment, while subtype 2 had milder symptoms, focusing on support and monitoring. These findings provide insights into TD classification and may help refine treatment strategies. However, the cross-sectional design limits causal interpretations, and reliance on parent-reported data may introduce bias.
Keywords: Clinical characteristics; Cluster analysis; Subtype classification; Tic disorder.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
