

Artificial intelligence driven 3D reconstruction for enhanced lung surgery planning
- PMID: 40312393
- PMCID: PMC12046031
- DOI: 10.1038/s41467-025-59200-8
Artificial intelligence driven 3D reconstruction for enhanced lung surgery planning
Abstract
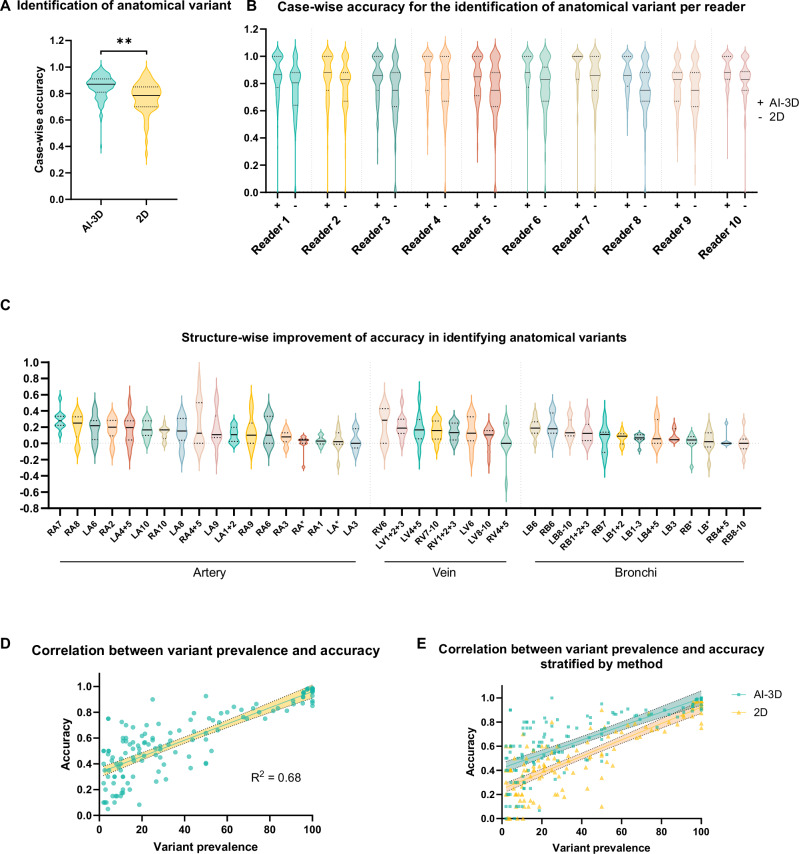
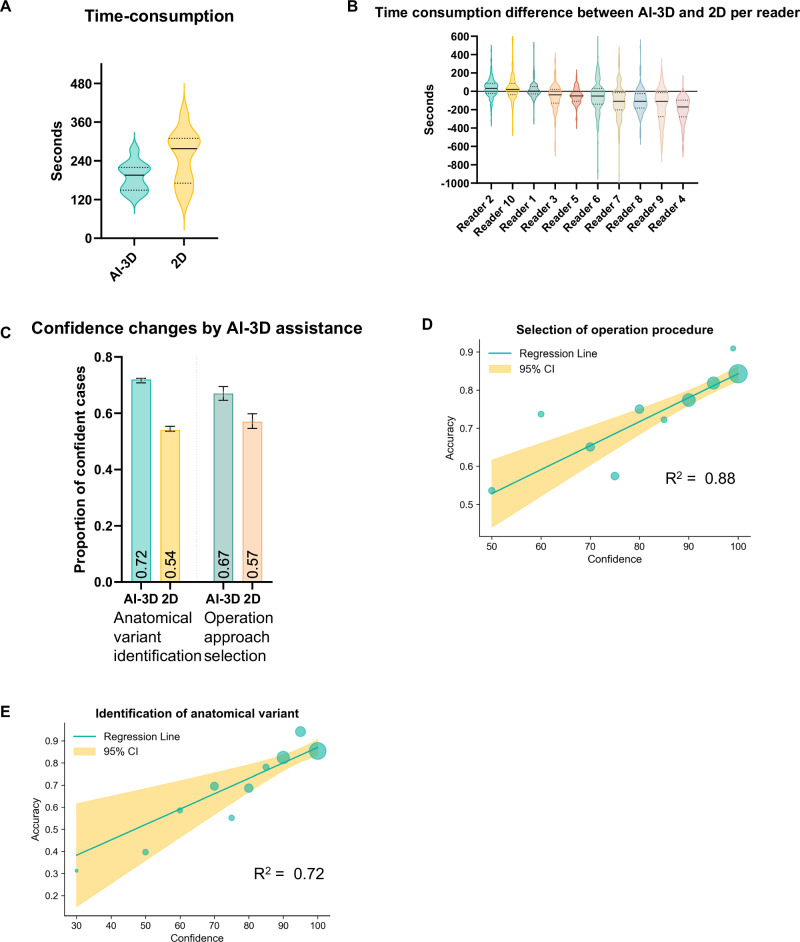
The increasing complexity of lung surgeries necessitates the need for enhanced imaging support to improve the precision and efficiency of preoperative planning. Despite the promise of 3D reconstruction, clinical adoption remains limited due to time constraints and insufficient validation. To address this, we evaluate an artificial intelligence-driven 3D reconstruction system for pulmonary vessels and bronchi in a retrospective, multi-center multi-reader multi-case study. Using a two-stage crossover design, ten thoracic surgeons assess 140 cases with and without the system's assistance. The system significantly improves the accuracy of anatomical variant identification by 8% (p < 0.01), reducing errors by 41%. Improvements in secondary endpoints are also observed. Operation procedure selection accuracy is improved by 8%, with a 35% decrease in errors. Preoperative planning time is decreased by 25%, and user satisfaction is high at 99%. These benefits are consistent across surgeons of varying experience. In conclusion, the artificial intelligence-driven 3D reconstruction system significantly improves the identification of anatomical variants, addressing a critical need in preoperative planning for thoracic surgery.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Dawei Wang, Chen Xia, Jinlong Liu, Bing Yang, Ji Qi, Fanghang Ji, Shaokang Wang are paid employees of Infervision Medical Technology Co., Ltd. The research was partially funded by Infervision Medical Technology Co., Ltd. The remaining authors declare no competing interests.
Figures


References
-
- Potter, A. L. P. T. et al. Assessing the number of annual lung cancer resections performed in the United States. Shanghai Chest7, 29 (2023).
-
- Siegel, R. L., Miller, K. D., Wagle, N. S. & Jemal, A. Cancer statistics, 2023. CA: a Cancer J. Clinicians73, 17–48 (2023). - PubMed
-
- Koch, R., Felsted, A. M., Virk, S., Roy, N. & Jayaraman, S. Surgical capacity building in low- and middle-income countries: lessons for thoracic surgery. Thorac. Surg. Clin.32, 269–278 (2022). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
