

Extracardiac Compression by Gastrointestinal Structures: A Comprehensive Anthology From the Literature
- PMID: 40313649
- PMCID: PMC12043395
- DOI: 10.1155/crp/5871029
Extracardiac Compression by Gastrointestinal Structures: A Comprehensive Anthology From the Literature
Abstract
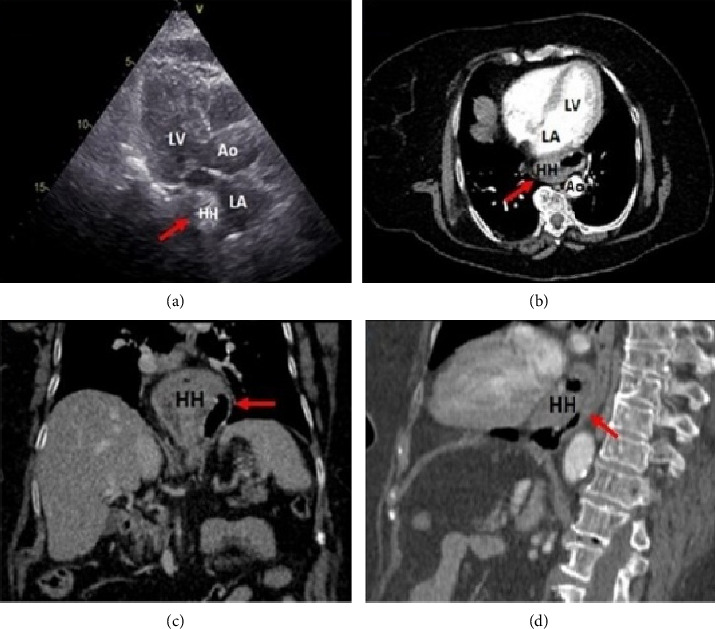
Extrinsic heart compression by gastrointestinal (GI) structures is an often underrecognized finding in clinical practice. It is potentially related to unpredictable clinical conditions, ranging from incidental detection in asymptomatic subjects, to deranging and potentially life-threatening clinical manifestations. However, despite its potential clinical relevance, there is still no comprehensive analysis investigating the surrounding causes, clinical findings, and diagnostic imaging work-up for this patient population. A narrative review with an extensive bibliographic search of the literature was performed using PubMed (MEDLINE), Embase, and Cochrane Central Databases up to December 31, 2023. Despite the broad spectrum of GI etiologies, clinical manifestations, and cardiac chamber involvement scenarios, physicians must be aware of such an uncommon condition, in order to provide timely diagnosis through a comprehensive imaging approach, avoid misleading interpretations, and determine the most appropriate decision-making strategy.
Keywords: ECG changes; clinical findings; extracardiac compression; gastrointestinal structures; imaging tools.
Copyright © 2025 Riccardo Scagliola et al. Cardiology Research and Practice published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
Publication types
LinkOut - more resources
Full Text Sources