

Chest computed tomography and plain radiographs demonstrate vascular distribution and characteristics in COVID-19 lung disease - a pulmonary vasculopathy
- PMID: 40313996
- PMCID: PMC12042850
Chest computed tomography and plain radiographs demonstrate vascular distribution and characteristics in COVID-19 lung disease - a pulmonary vasculopathy
Abstract
Introduction: Early in the COVID-19 pandemic, CT was demonstrated as a sensitive tool for diagnosing COVID-19. We undertook a detailed study of CT scans in COVID-19 patients to characterise disease distribution within lung parenchyma, respiratory airways, and pulmonary vasculature, aiming to delineate underlying disease processes.
Methods: We characterised acute phase chest CT of 40 participants with COVID-19 from the REACT study, 31 with CT pulmonary angiography (CTPA), 4 with intravenous contrast enhanced CT and 5 with non-intravenous contrast enhanced CT. Participants had neither been vaccinated nor received systemic steroids. We further correlated the distribution of lung parenchymal damage on CT with contemporaneous chest radiographs.
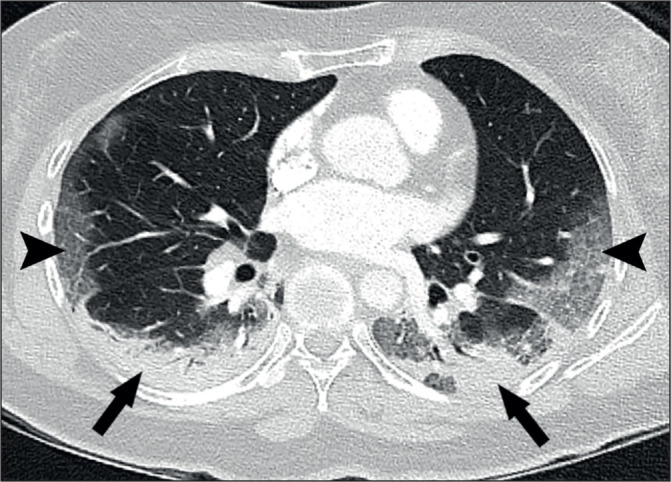
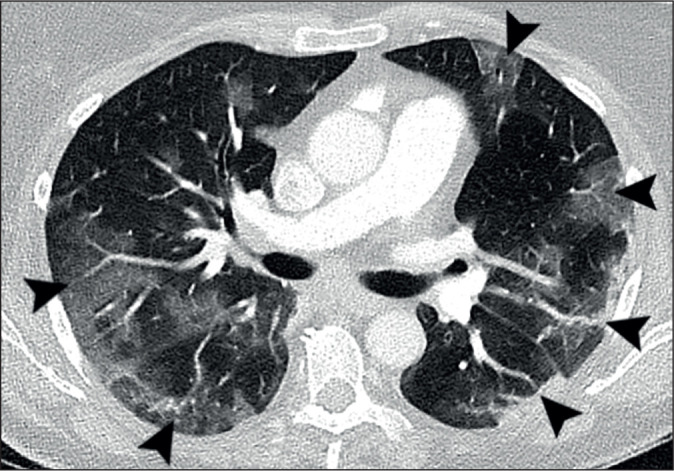
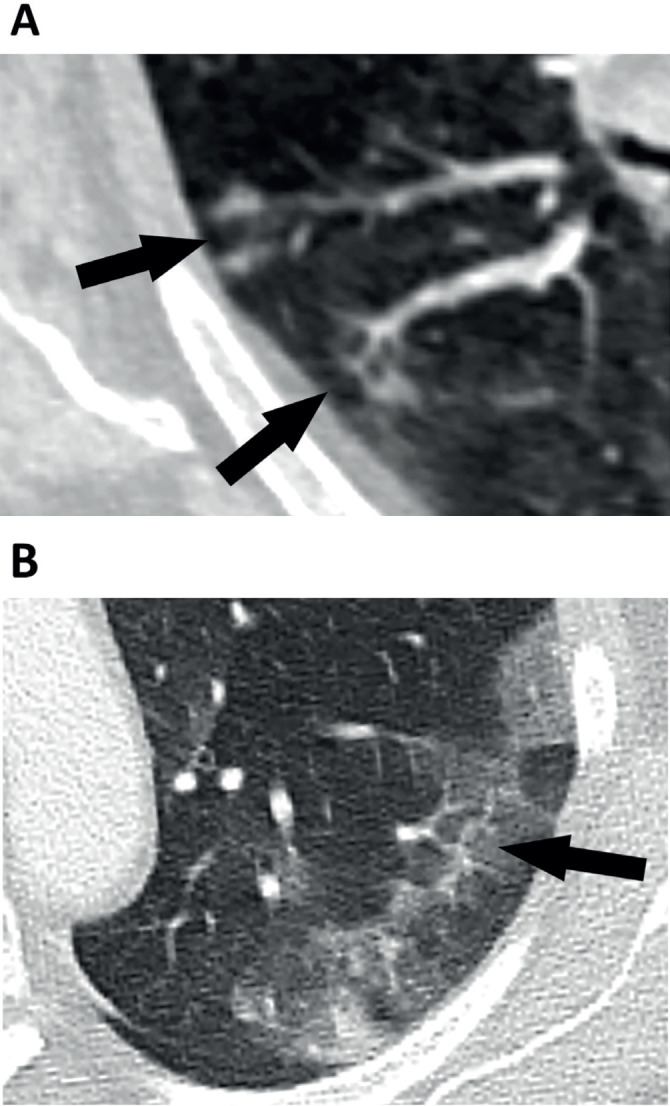
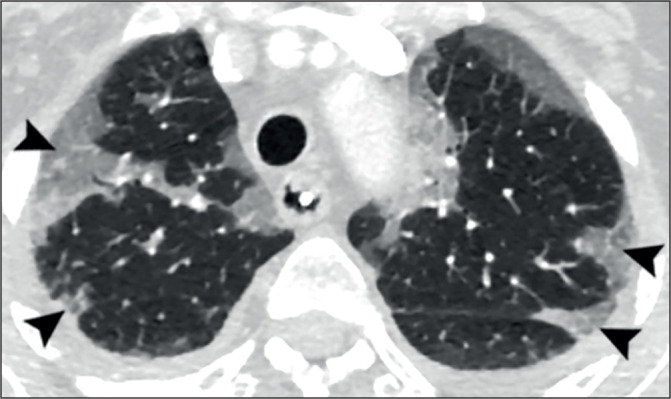
Results: Parenchymal lung damage was found in all subjects. However, airways inflammation was present in only 23% (9) and limited to small areas. Notably, vascular abnormalities were dominant and characterised by dilated peripheral pulmonary vessels supplying areas of lung damage in a gravity-dependent distribution bilaterally in 95% (38), basally in 90% (36), peripherally in 92.5% (37), and posteriorly in 90% (36). Macrothrombosis was demonstrated in 23% (7) of CTPAs. Wedge-shaped peripheral lung damage, resembling areas of pulmonary vascular congestion, were distinct in 53% (21) with or without visible macrothrombosis. Pleural effusions were seen in 28% (11). Notably, lung opacification distribution in 98% of the plain radiographs matched distribution on CT (39).
Conclusion: Our study frames COVID-19 as a pulmonary vasculopathy rather than a more conventional pneumonia which may be important not only for guiding mechanistic study design but also for the development of novel targeted therapeutics.
Keywords: COVID-19; CT imaging; Chest Radiographs; Respiratory Infections; Vasculopathy.
Copyright © 2025 Ulster Medical Society.
Figures

Similar articles
-
Imaging features of the initial chest thin-section CT scans from 110 patients after admission with suspected or confirmed diagnosis of COVID-19.BMC Med Imaging. 2020 Jun 15;20(1):64. doi: 10.1186/s12880-020-00464-5. BMC Med Imaging. 2020. PMID: 32539692 Free PMC article.
-
Preoperative examination of lung transplant candidates: value of chest CT compared with chest radiography.AJR Am J Roentgenol. 1995 Dec;165(6):1343-8. doi: 10.2214/ajr.165.6.7484560. AJR Am J Roentgenol. 1995. PMID: 7484560
-
Typical Imaging Patterns in COVID-19 Infections of the Lung on Plain Chest Radiographs to Aid Early Triage.Rofo. 2021 Oct;193(10):1189-1196. doi: 10.1055/a-1388-8147. Epub 2021 Mar 10. Rofo. 2021. PMID: 33694145 English.
-
Coronavirus Disease 2019 (COVID-19) Pneumonia Presentations in Chest Computed Tomography: A Pictorial Review.Curr Probl Diagn Radiol. 2021 May-Jun;50(3):436-442. doi: 10.1067/j.cpradiol.2020.06.010. Epub 2020 Jun 27. Curr Probl Diagn Radiol. 2021. PMID: 32839069 Free PMC article. Review.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 16;3:CD013639. doi: 10.1002/14651858.CD013639.pub4. PMID: 33242342 Updated.
References
-
- Adam EJ, Grubnic S, Jacob TM, Patel JH, Blanks R. COVID-19: could CT provide the best population level biomarker? Incidental COVID-19 in major trauma patients suggests higher than predicted rates of infection in London. Clin Radiol. 2021;76(1):74.e15–74.e21. doi: 10.1016/j.crad.2020.10.008. - DOI - PMC - PubMed
-
- Ali TF, Tawab MA, ElHariri MA. CT chest of COVID-19 patients: what should a radiologist know? Egypt J Radiol Nucl Med. 2020;51(1):120. doi: 10.1186/s43055-020-00245-8. Epub 2020 Jul 7. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical