

Induced B cell receptor diversity predicts PD-1 blockade immunotherapy response
- PMID: 40314973
- PMCID: PMC12067265
- DOI: 10.1073/pnas.2501269122
Induced B cell receptor diversity predicts PD-1 blockade immunotherapy response
Abstract
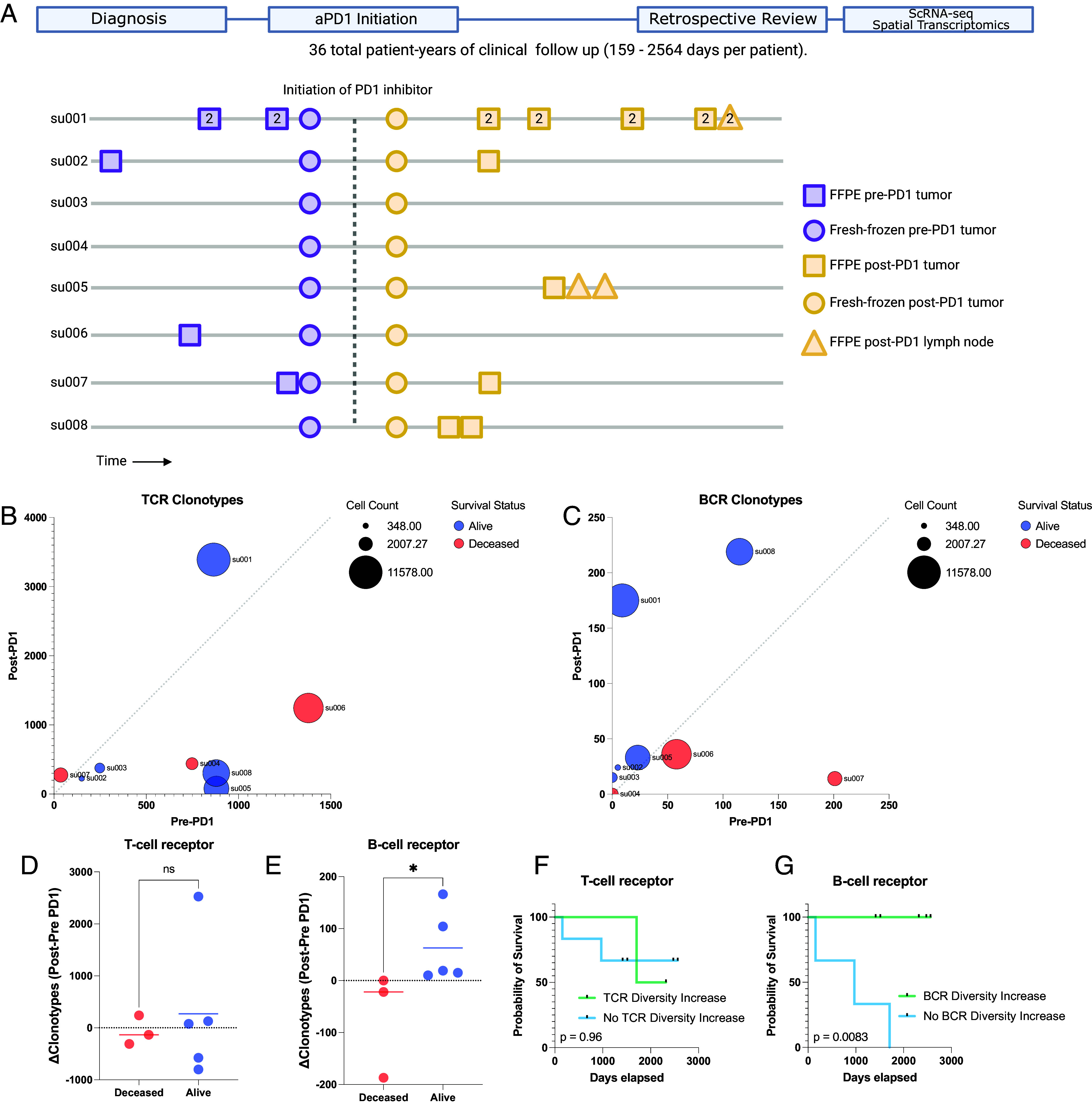
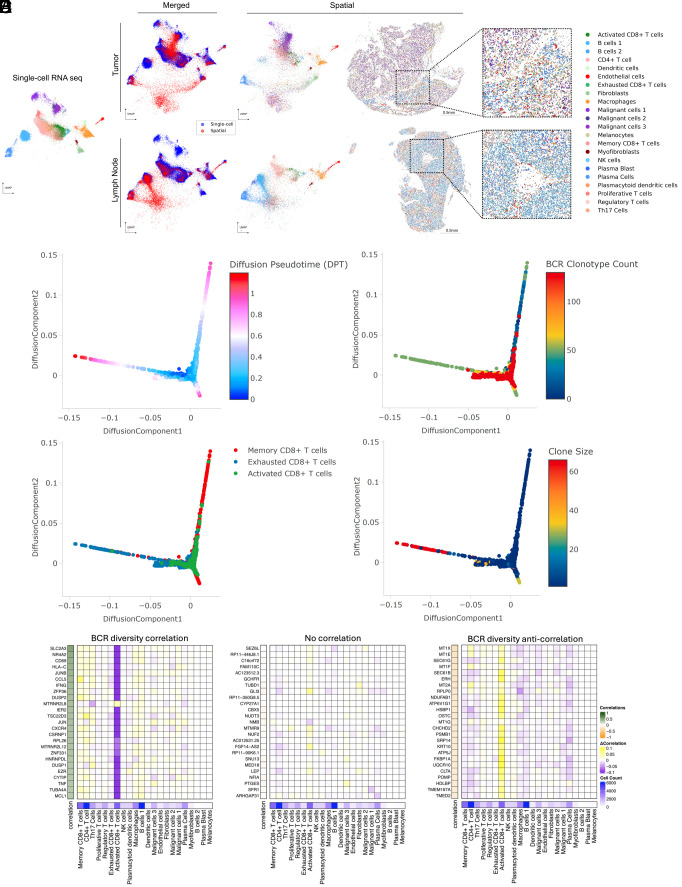
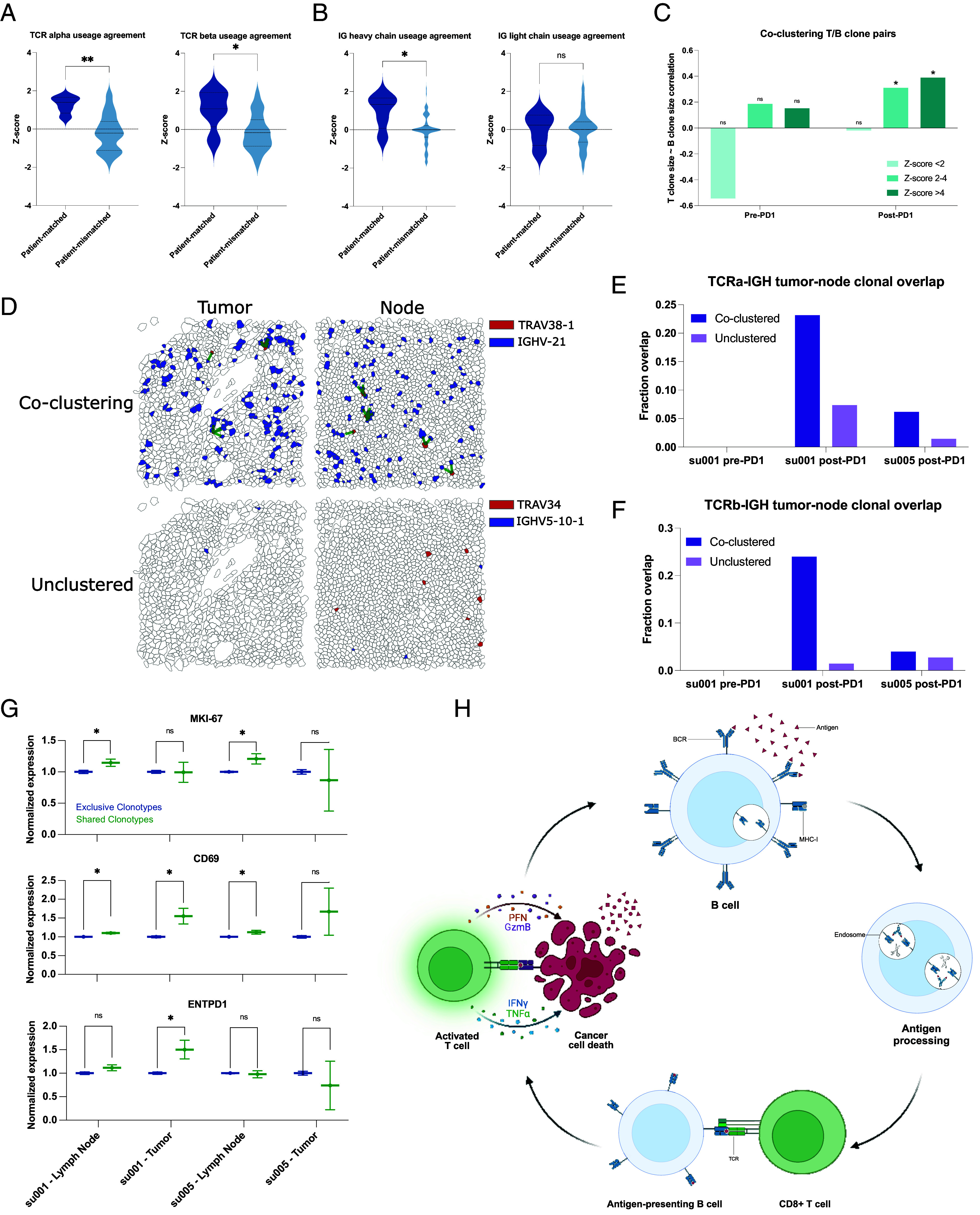
Immune checkpoint inhibitors such as anti-Programmed Death-1 antibodies (aPD-1) can be effective in treating advanced cancers. However, many patients do not respond, and the mechanisms underlying these differences remain incompletely understood. In this study, we profile a cohort of patients with locally advanced or metastatic basal cell carcinoma undergoing aPD-1 therapy using single-cell RNA sequencing, high-definition spatial transcriptomics in tumors and draining lymph nodes, and spatial immunoreceptor profiling, with long-term clinical follow-up. We find that successful responses to PD-1 inhibition are characterized by an induction of B cell receptor (BCR) clonal diversity after treatment initiation. These induced BCR clones spatially colocalize with T cell clones, facilitate their activation, and traffic alongside them between tumor and draining lymph nodes to enhance tumor clearance. Furthermore, we validated aPD-1-induced BCR diversity as a predictor of clinical response in a larger cohort of glioblastoma, melanoma, and head and neck squamous cell carcinoma patients, suggesting that this is a generalizable predictor of treatment response across many types of cancers. We find that pretreatment tumors harbor a characteristic gene expression signature that portends a higher probability of inducing BCR clonal diversity after aPD-1 therapy, and we develop a machine learning model that predicts PD-1-induced BCR clonal diversity from baseline tumor RNA sequencing. These findings underscore a dynamic role of B cell diversity during immunotherapy, highlighting its importance as a prognostic marker and a potential target for intervention in non-responders.
Keywords: PD-1 inhibition; basal cell carcinoma; cancer; immunotherapy; spatial transcriptomics.
Conflict of interest statement
Competing interests statement:H.Y.C. is a cofounder of Accent Therapeutics, Boundless Bio, Cartography Biosciences, Orbital Therapeutics. H.Y.C. was an advisor of Arsenal Biosciences, Chroma Medicine, Exai Bio and Spring Science until December 15, 2024. H.Y.C. is an employee and stockholder of Amgen as of December 16, 2024. H.Y.C. was on the Scientific Advisory Board of Arsenal Bio (2019 to 2024), where one reviewer Z.Z. currently works. This work was was submitted for publication after H.Y.C.’s relationship with Arsenal Bio ended. A.L.S.C. has served as a clinical investigator and/or consultant for Merck, Regeneron, Sun Pharma, Feldan, and Castle Biosciences. A.T.S. is a founder of Immunai, Cartography Biosciences, Santa Ana Bio, and Prox Biosciences, an advisor to Zafrens and Wing Venture Capital, and receives research funding from Astellas and Northpond Ventures. The remaining authors declare no competing interests.
Figures


Update of
-
Induced B-Cell Receptor Diversity Predicts PD-1 Blockade Immunotherapy Response.bioRxiv [Preprint]. 2024 Dec 4:2024.12.03.626669. doi: 10.1101/2024.12.03.626669. bioRxiv. 2024. Update in: Proc Natl Acad Sci U S A. 2025 May 6;122(18):e2501269122. doi: 10.1073/pnas.2501269122. PMID: 39677742 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
